
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease, with cervical spine instability being one of its consequences. Joints in the cervical section of the spine, according to the literature, are the third to be involved by the disease, after joints of the hands and feet [1].
According to Garrod, who in 1890 was the first to describe the involvement of the joints of the cervical spine, they are present in approx. 35% of the patients; according to our data, radiological changes are observed in over 80% of the patients [2, 3].
Inflammation in RA leads to the damage of articular cartilages, compact bone erosion, and weakened ligaments, being a great environment for biomechanical balance disorders in joints at different levels of the spine [1]. The course of the destruction process in the joints may be asymptomatic or manifesting with strong pain. Neurological disorders are present in 7–35% of the patients [2].
In extreme cases, cervical spine instability leads to death as a result of spinal cord compression [4, 5]. Treating patients with cervical spine instability and accompanying low quality of bones is a serious issue. Sagittal balance is one of the issues that has recently contributed to deepening the understanding of spine pathology [6].
It has been observed that sagittal balance correlates to the quality of patients’ lives and is a prognostic factor as regards the effects of surgical procedures [7, 8]. The application of sagittal balance principles in daily surgical practice has significantly improved management outcomes as regards patients suffering from ailments in the lumbar and thoracic spine [9, 10].
Fewer papers have so far been published on the understanding and application of sagittal balance in the pathology of the cervical spine [11, 12]. Few publications concern the topic of sagittal balance in patients with instability in the course of RA [13].
The goal of the paper is to draw the attention to selected parameters of the sagittal balance and their mutual relations, as regards cervical spine, as well as to provide diagnostic and therapeutic guidelines to rheumatologists and orthopaedists dealing in everyday practice with patients suffering from RA.
Cervical spine instability in rheumatoid arthritis
The joints of the cervical spine are rich in synovial membrane and are predisposed to the development of inflammatory changes in the course of RA. The anatomy, particularly of the upper cervical spine, is characterised by large mobility and no natural osseous stabilisation [14].
As a result of inflammation and mechanical factors, the complex connective tissue system loses its stability. Among other things, the transverse ligament of the atlas, while losing strength, causes widening of the atlantodens interval (ADI). Atlanto-axial subluxation (AAS) is then created. Damage to the conoid ligaments deepens the AAS, resulting in the atlas slipping downwards and to the front, thus decreasing the posterior atlas and dens interval (PADI). The apex of dens penetrates to the foramen magnum (cranial settling – CrS).
Within the subaxial area C2–C7, excessive dislocation of the bodies towards each other and instability of subaxial subluxation (SAS) results both from the destruction of articular surfaces of the adjoining bodies, weakened ligaments between the spinous processes, and destruction of the intervertebral discs connecting the adjoining bodies.
Atlanto-axial subluxation is present in 65% of the patients with RA, 75% of all the AAS being anterior subluxations (approx. 75% of all the AAS); posterior and lateral ones are not as common. Subluxations in C3 through C7 vertebrae (SAS) are described in approx. 20%, while axial dens herniation to the foramen magnum CrS are seen in approx. 15% of the cases in patients with RA [12, 14, 15]. Inflammation in RA may cause erosion of the axial dens and its fracture [16].
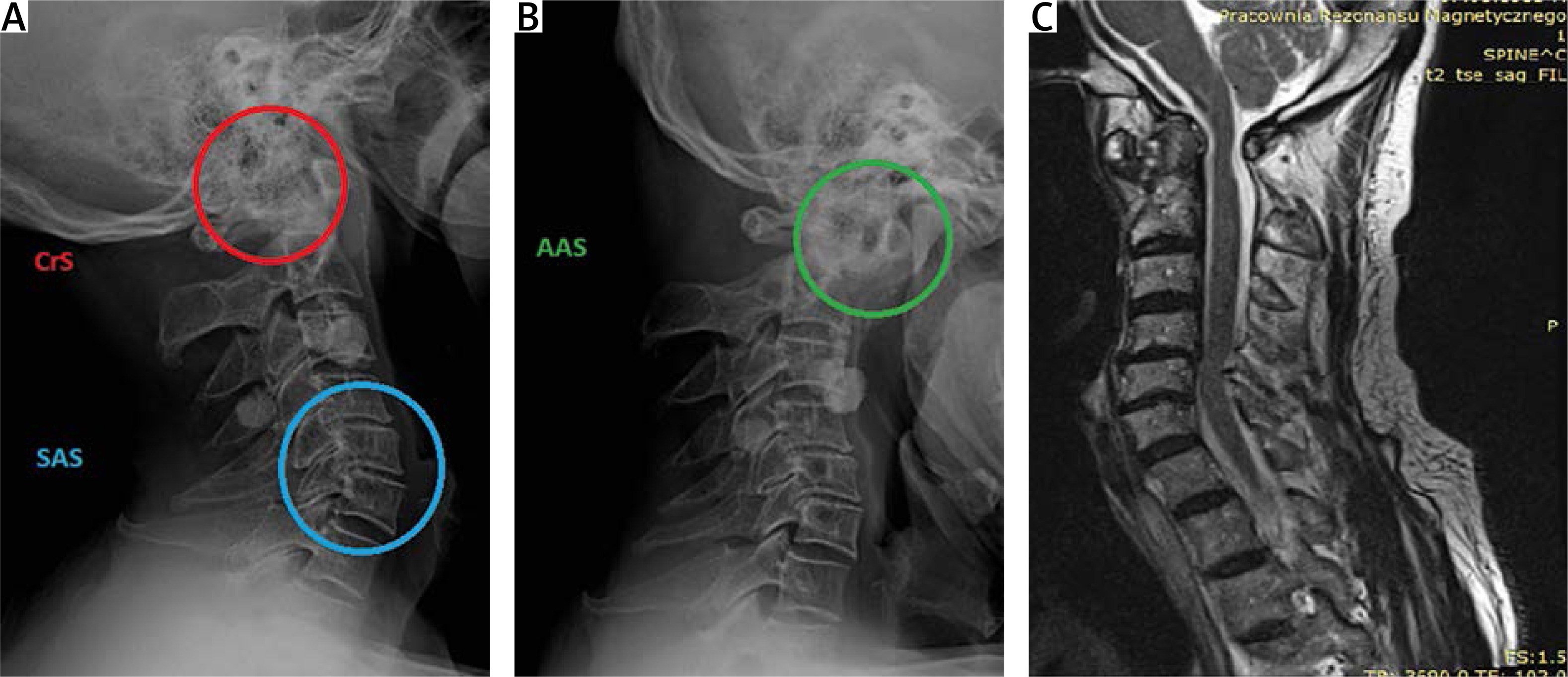
Lack of connective tissue protection at the above levels may lead to compression on the nerve structures, but also the vessels, leading, e.g., to cerebral thrombosis. Diagnostic imaging in the majority of patients with RA, also without any clinical signs of instability, comprises X-ray of the cervical spine AP and lateral, classical and functional. Assessments make it possible to evaluate the structure of the bones and mutual relations. In the case of neurological changes, even in the case of lack of irregularities upon X-ray, it is necessary to have magnetic resonance imaging or computed tomography carried out (Fig. 1).
Fig. 1
Lateral X-ray of the neck of a 67-year-old patient with rheumatoid arthritis and instability of cranial settling, atlanto-axial subluxation, subaxial subluxation (A), X-ray of the patient’s neck in anteversion (B), magnetic resonance imaging of the neck of the patient made before the planned surgery (C).
Regional radiological classifications were drawn up specifying the range of standards and degrees of instability based on the assessments of healthy subjects and ill ones. In cranial settling assessment they are Ranawat classification, Redlund-Johnell criterion, Clark classification, ADI, PADI in AAS value assessment, or assessment of the rate of body displacement and the assessment of vertebral canal diameter in SAS [14, 15].
Classifications applied in the clinical evaluation of myelopathy in RA comprise the Ranawat classification [17] and the classification of the American College of Rheumatology assessing the general functional condition of the patient suffering from RA [3].
It is worth emphasising the fact that neurological clinical signs proving the compression of nerve structures may create interpretation difficulties due to the occurrence in the natural course of RA of limitation in the range of motion, contractures, and weakened muscles.
The notion of an efficiency conus, kinematic chain and global sagittal balance
Dubousset is among the leaders of studies on sagittal balance [18]. According to Dubousset, sagittal balance is a balanced ratio of all the curvatures of the spine (kyphosis, lordosis), which is aimed at keeping the position of the body in space against gravity and economically using as little energy as possible. The position of the body has to simultaneously maintain, as well as the balance, the location of the skull, which enables optimum horizontal field of view [18, 19].
A human body is compared to a chain of kinematic constituents, which are affected by equilibrant forces and moments of force [20]. It begins with the support polygon of the feet, later continuing into the ankle joints, knee joints, hip joints, and pelvic girdle, and then through spinal segments to the cervical section and the head. The axes for muscle operation are joints, which in the case of destruction hinder the action of equilibrant forces.
According to the principles of Dubousset’s theory, sagittal alignment of the spinal curvatures must be included in the “efficiency conus” [18]. Global sagittal balance is the condition where the location the skull, spine, pelvis, and lower limbs is consistent in order to have an ergonomic posture. This translates into the course of the body line of gravity, the projection of which should be included in the support polygon of the feet.
An optimum course of the line of gravity is the course from the centre of gravity of the head, through the centre of the C2 body, C7 body, femoral head, and through extension of the knee joints to the base area specified by the location of the feet. Such a course of the line of gravity is not common in patients with an advanced RA. Deviations from the optimum condition result in the activation of compensation mechanisms at various levels of the kinematic chain, using up additional energy [21, 22].
Imaging devices coupled with a movement platform are used for specialist assessment concerning body balance in space [23]. However, in everyday clinical practice, the evaluation of sagittal balance parameters translates into static X-rays [24]. The radiological parameters of the evaluation are as follows:
projections of centre of gravity points of the selected parts of body on the surface area of the support polygon of the feet (vertical sagittal lines),
geometry and spatial orientation of the head making optimum field of vision possible,
spatial, segmentary, regional, and global orientation of the spine curvatures,
geometry and spatial orientation of the sacrum and pelvis,
geometry and spatial orientation of lower limb joints.
Each parameter has standard values, which were described in the literature based on multiple studies of healthy and ill subjects [25, 26].
Regional radiological parameters of sagittal balance
Skull
The skull is the highest located element of the body. According to Dubousset [18], the skull – despite its morphological differences – may be treated as the “cephalic vertebra”.
As regards the X-ray diagnostics, to assess the sagittal balance of the skull, parameters described as permanent (not changing after adolescence) will be of help as well as the parameters that are independent of the advancement of the person’s life, namely variables whose value depends on the orientation of the skull in the space (Table I), (related to spatial orientation of the head, for which it is natural to aim to have a position ensuring an optimum range of horizontal field of vision and balance).
Table I
Radiological permanent parameters and radiological temporary parameters within the skull
Cervical spine
The mobility of the cervical spine is responsible for keeping the head over the body and a horizontal field of vision. The weight of the head is transferred by the occipital condyles of the cranium to the lateral masses, where through joints C1–C2 to C2, dividing the load of C2 to the anterior column (36% of the load) and 64% of the load to the posterior column.
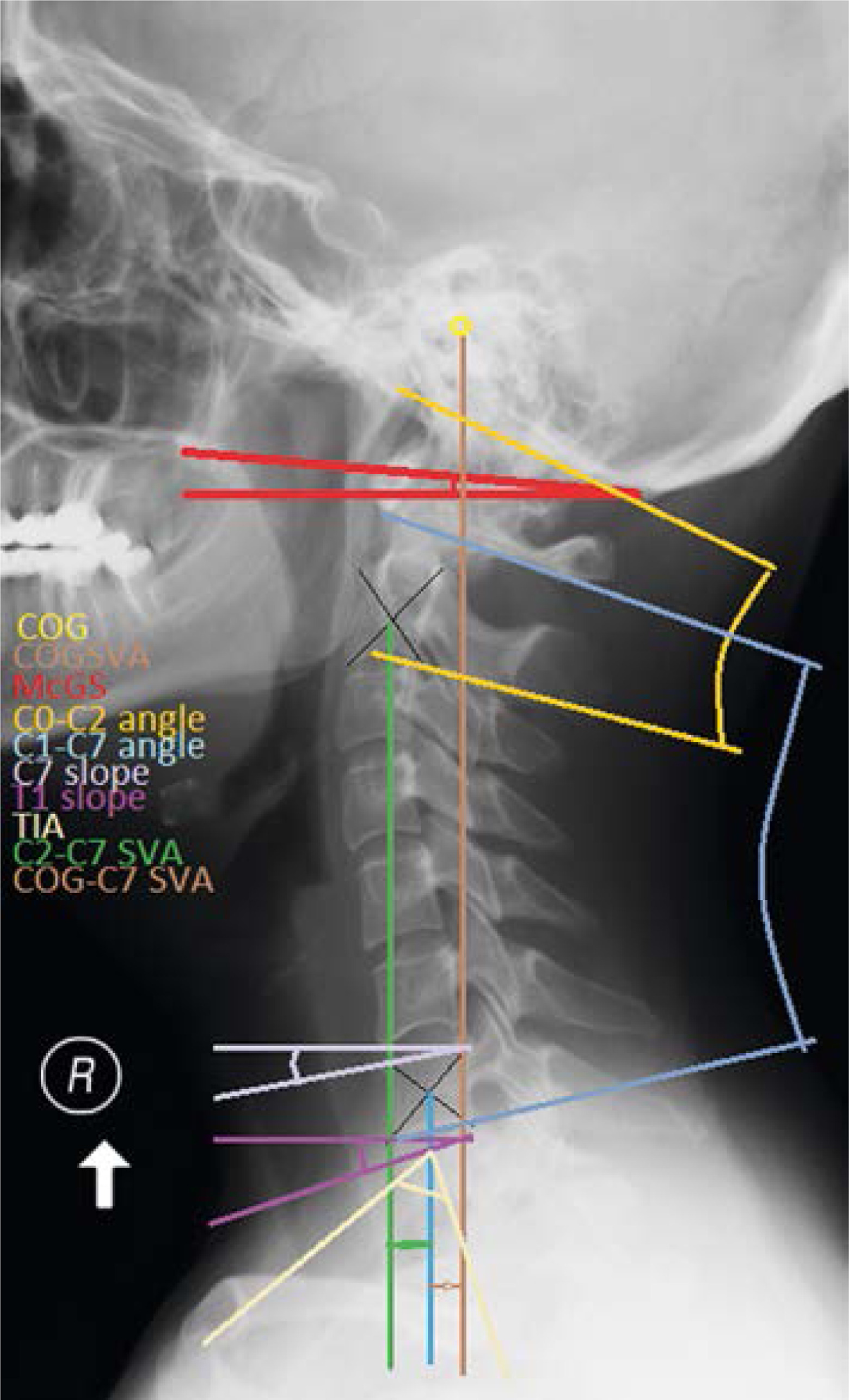
A similar course of load is present down to C7 [27]. Large mobility of the cervical section and the compensation mechanisms inside it hinder the definition of unquestionable normative parameters. At present, the selected determined parameters of sagittal balance evaluation of the cervical spine are presented in Figure 2 and Table II.
Table II
Radiological parameters in the cervical spine
Sagittal balance parameters
As regards the papers on spine balance, the greatest advancement in the knowledge was observed in the field of quantitative evaluation methods, standards, and disorders in pelvis biomechanics, the lumbosacral section, and the thoracic section. After a period of studies on the regional parameters of spine assessment, there have been papers describing the inter-regional dependencies, their impact on the pathogenesis of diseases, and the quality of life [28–30].
The key paper was that of Duval-Beaupère et al. [31], describing 3 parameters determining the shape and location of the pelvis in the sagittal plane and their strict correlation with the parameters of the adjoining lumbar spine. The paper was the basis for the modern understanding of sagittal balance commonly used nowadays in lumbar and thoracic spine surgery.
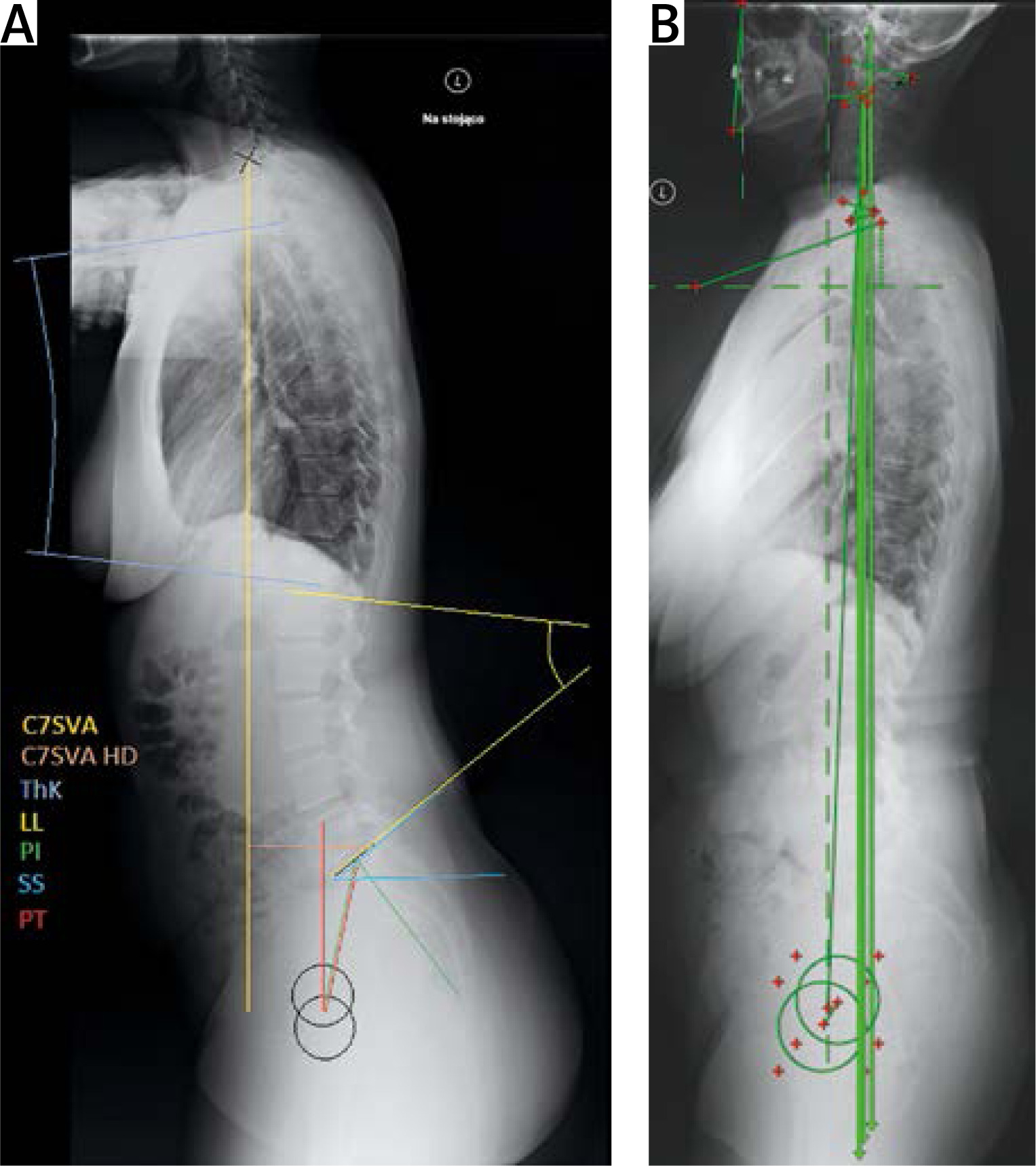
Treating the pelvis as a solid mass, a permanent parameter was observed, which does not change after adolescence, i.e. pelvic incidence, and variable parameters depending on the location of the pelvis in the sagittal plane pelvic tilt and sacral slope. Inter-regional relations between the pelvis and the sacrum and the lumbar, thoracic section as regards the equilibrium and the course of the sagittal vertical axis (SVA) taken from the body of C7 vertebra were defined as the “sagittal balance of the spine” (Fig. 3, Table III).
Table III
Basic radiological parameters within the thoracic, lumbar, and sacral section and the pelvis
Lower limbs
The spine cannot be treated as an isolated element. The next levels of balance compensation are joints of the lower limbs, such as: hip, knee, and ankle joints. Movement and spatial orientation at particular levels are of particular importance for patients with RA, for whom, during the natural course of the disease, there is an impairment of peripheral joint functioning and the chain of equilibrant forces due to contractures and joint deformation [32, 33].
Impairment in the functioning of peripheral joints limits their role in balance compensation and may result in additional load to the axial joints, including the ill minor joints of the cervical spine. The aim of the paper limits the scope down to the relation between the cervical section and adjoining regions.
Relation between the sagittal balance and the selected parameters of the cervical spine
Studies on RA focus on the one hand on the aetiology of the disease and identification of the factors predisposing to its advancement, and on the other hand on the improvement of diagnostics, widening the scope of conservative treatment and surgery [3, 6, 14].
The literature presents a few papers devoted to the sagittal balance in RA. One of them is the paper by Masamoto et al. [34], describing the correlations between the sagittal balance and other factors affecting the course of RA, such as activity of the disease, bone mineral density, and treatment with glucocorticosteroids.
Other papers by Lee et al. [8] and Mochizuki et al. [35] describe the relation of the selected sagittal balance parameters with the quality of life in RA patients. Cervical spine plays a key role in behaviour and positioning of the head in a way, making assessment of the environment the most favourable; it also transfers the weight related to balance and keeping the head over the body.
This is possible along with the aim to perform one of the basic features and functions of the spine, i.e. efficient balance and concentricity. Keeping the body in a static and dynamic balance in space is possible thanks to compensation mechanisms present in the links of the kinematic chain [20, 36].
Cervical spine instability in patients with RA occurs after having used up all the complex compensation mechanisms covering balancing the forces and their moment, in the spine, the pelvis, and the lower limbs. The majority of past papers on balance cover the thoracic and lumbosacral sections and the pelvis [9, 37, 38].
Based on the studies carried out due to other ailments of the spine, it may be observed that the particular regions of the spine and links of the kinematic chain are not independent from one another, and there are multiple significant and close correlations. The parameters that cover the cervical section and show graphically the concentricity of the spine are the sagittal planes from point C2, C7 and from the centre of gravity of the head (COG) [33, 38–40].
Physiologically speaking, the centre of gravity of the head is above the centre of the dens of the C2 body. The course of the COG, SVA, C2SVA, and C7SVA reflects the global and segment balance. In practice, SVA translation may imply clinical consequences. The relation between the dislocation of C2SVA towards C7SVA has been proven along with worsening HRQoL of the patients [41–43].
Another parameter of global balance covering also the cervical section is the odontolit hip axis (OD-HA) [44]. The angle between the line connecting axis dens and the centre of the section connecting the femoral heads and the vertical line going through the centre of the line connecting femoral heads. If the OD-HA is over +2 degrees, or below –5 degrees, the lever arm as regards the force in action is too big and has clinical implications [45, 46].
Clinical implications at the level of the relationship between the particular segments of the spine is included in the thoracic inlet tilt concept. Lee et al. [47] presented in their paper the concept of a thoracic inlet tilt as being strictly correlated to the cervical spine balance. The concept was based on a similar one present in the lumbar section.
A relationship between cervical lordosis (CL) and C-Th transition anatomy was observed, similarly to lumbar lordosis (LL) and pelvic anatomy. Th1 starts at the thoracic inlet, the girdle of which also includes the ribs and the upper sternal line. The area is a transition of the movable cervical section into a stiff thoracic spine. S=The sagittal setting of the cranium and cervical spine may have an impact on upright posture and horizontal field of vision (chin-brow vertical angle – CBVA), similarly to the relationship between the position of the pelvis and the lumbar spine.
Lee et al. [47] and Knott et al. [48] state in their paper a significant relationship between the thoracic inlet angle Tslope and the relocation of the skull and craniovertebral flattening. The position of the skull and the cervical spine is forced by the strive to have a horizontal field of vision, it impacts the compensation global setting of the spine and pelvis. There was a correlation of incidence of pelvis and LL observed while studying the relationship between particular sections of the spine.
Also, correlation has been found as regards LL and thoracic kyphosis as well as thoracic kyphosis and CL. No correlation was observed between the incidence of pelvis and thoracic kyphosis, which complicates the course of the abovementioned kinematic chain of correlations from the pelvis to the cervical spine [12].
This shows that thoracic kyphosis does not result from lumbar lordosis, but rather LL is the result of thoracic kyphosis and pelvic statics. Likewise, it may be assumed that CL results from the spatial orientation of the skull and thoracic kyphosis. The adjoining stiff thoracic segment and the skull, along with an impaired ligament system of the cervical spine in the course of RA, may particularly foster changes comparable to adjacent segment disease (ASD) [49, 50].
A similar phenomenon is observed adjacent to pathologically fused vertebrae and following some spine stabilisation surgeries [51–54]. Compensation disorders also cause the body to be positioned towards the efficiency conus circumference, which results in increased energy used to keep balance; when lasting for a longer time, it results in tiredness, muscle pain, weakness, or in the case of damage to articular surface also joint subluxation and pressure on the adjoining structures. The order of the above-described sequences damaging the ligament system causing CrS, atlanto-axial subluxation, and SAS instability seems not to be random and requires further evaluation
Evaluation of the sagittal balance of the spine is currently one of the basic elements of planning spine disease management, which guarantees improvement in the patients’ quality of life. In the case of patients suffering from RA, due to the course of the disease, evaluation of the body balance parameters is of particular importance [55].
While planning the management in the case of patients with features of instability, postural assessment is recommended along with sagittal balance evaluation. The assessment of the cervical spine uses such parameters as CBVA, nasion-inion line, COGSVA, C2SVA, C7SVA, C2–C7 translation, SVA, CL, T slope, transient ischaemic attack, and OD-HA. Postural assessment evaluates whether we are dealing with natural instability or a secondary one related to the pathology below the cervical spine.
This impacts the management strategy. In the case of the decision to perform a surgery, this will allow planning of an optimum procedure minimising complications, such as destabilisation and ASD.
Conclusions
The literature draws too little attention to sagittal balance in patients suffering from RA; however, the importance of surgical procedures in instability of that section before neurological deficits occur is emphasised, as a prevention.
Postural assessment of the spine is the basic element of cervical spine instability in RA diagnostics, as well as a functional test of the cervical spine.
Total assessment of spatial orientation of the skull, cervical spine alignment parameters, and sagittal balance is an important element in planning the surgery of cervical spine instability in RA.
Knowledge on the relation between cervical spine instability in patients suffering from RA, sagittal balance, and the remaining elements of the kinematic chain of the body is still insufficient and requires further studies.