
Introduction
Joint involvement is one of the most common manifestations of various systemic connective tissue diseases (CTD). It affects about 15–90% of patients with primary Sjögren’s syndrome (pSS) [1], 69–95% of patients with systemic lupus erythematosus (SLE) [2, 3], 46–97% of patients with systemic sclerosis/scleroderma (SSc) [4] and about 89–100% of patients with mixed connective tissue disease [5].
In CTD, joint involvement can have diverse manifestations, from arthralgia and non-destructive arthritis to destructive arthritis that can lead to permanent disability.
Moreover, overlapping of locomotor manifestations with musculoskeletal symptoms, which may occur in the course of coexistent osteoarthritis, fibromyalgia or mood swings often observed in CTD, are a frequent problematic issue. This problem concerns about 50% of patients with pSS and 30% of patients with SLE [6].
Because of a great variety of articular manifestations in the course of CTD, it is essential to find the right tool to obtain reliable assessment of severity of the musculoskeletal involvement so that proper decisions about more insightful diagnostics and intensification of treatment, or about referring the patient to another specialist (orthopaedist, psychiatrist), can be made.
In order to assess the degree of joint involvement in the course of CTD, an attempt is made to use indices that are routine tools in the assessment of arthritis activity in rheumatoid arthritis (RA).
They include the original 44-joint disease activity score (DAS), DAS28–ESR (erythrocyte sedimentation rate – ESR), DAS28–CRP (C-reactive protein – CRP), Simplified Disease Activity Index (SDAI) and Clinical Disease Activity Index (CDAI) [7]. The scales recommended for SLE, e.g. the Systemic Lupus Erythematosus Disease Activity Index Scale (SLEDAI) or British Isles Lupus Assessment Group (BILAG), are also applied [8].
Even though various tools for assessment of the activity of articular inflammatory diseases are available, appropriate determination of the degree of joint involvement is difficult because of wide symptomatology and frequently a severe course of diseases such as SLE, pSS or SSc (kidney, central nervous system, respiratory system or cardiovascular system – CVS, involvement).
It must be remembered that proper evaluation of joint involvement in the course of CTD has an immense effect on the overall assessment of the disease activity since it will give grounds for timely implementation of appropriate treatment and making a further prognosis.
Methods of assessment of inflammatory activity in the joints in the course of connective tissue diseases
Irrespective of the type of CTD, joint involvement is a substantial clinical problem which may lead to significant deterioration of the quality of life as well as irreversible bone destruction resulting in disability. Moreover, in many cases, joint changes in the course of CTD are an independent factor of poor prognosis and they are connected with involvement of other bodily organs and systems; they may also be suggestive of exacerbation of the course of the underlying disease.
What tools for evaluating inflammatory activity of the joints do we have at our disposal then? The scales used to assess RA activity are partly the tools, while the others are disease activity assessment scales which are used in particular systemic CTD, where the articular component is one of the scale components.
The most important characteristics of the scales used for disease activity assessment include adequate psychometric properties such as reliability, clinical relevance or appropriate response to changes in disease activity. Additional important aspects determining the use of appropriate scales are their low cost and easy application in everyday practice – such a tool should not be time-consuming or complicated, should not require specialist equipment, and should be easy to interpret [9].
Although with a different degree of reliability, most of the scales used to assess RA activity may also be used to evaluate the locomotor involvement in the course of CTD. These scales typically consist of several components and they include questionnaires and scales completed by both the patient and physician, physical examination of the joints, laboratory tests and also, though more seldom, imaging test results.
The most common patient-completed scales include the Visual Analogue Scale (VAS) for pain or disease activity assessment, the Numerical Rating Scale and the Health Assessment Questionnaire (HAQ) [10, 11].
The Health Assessment Questionnaire scale is divided into 8 sections evaluating everyday activities (getting up, dressing, eating, walking, personal hygiene, reaching for objects, grasping objects and activities. Each section usually contains 2 or 3 questions and, depending on the degree of functional capacity, the patient scores 0–3 points.
In addition, while rating each section, the use of assistive devices or other people’s assistance is also taken into consideration (assistive device – 1 extra point; people’s assistance – 2 points; both forms of assistance – 3 points). The highest rating determines the score in a given category and the total number of points is divided by 8. The final result is 0–3 (the higher the score, the more advanced the health deterioration) [11].
On physical examination of the joints, which is an important component, joint tenderness and swelling are evaluated. Most frequently, 28 joints are examined, i.e. small joints of the hand, such as proximal interphalangeal (PIP) joints and metacarpophalangeal (MCP) joints, also the wrist, elbow, shoulder and knee joints; in some cases, 44 joints may be evaluated (additionally: the MCP joints of the foot, sternoclavicular joints, acromioclavicular joints as well as the ankle joint) or, in the case of tenderness, 68 joints, and in the presence of swelling, 66 joints [12–14].
Joint tenderness may also be determined by means of a semi-quantitative method, i.e. with the Richie index, a component of the original DAS Scale. In this case, 52 joints are evaluated for tenderness and they include: the shoulders, elbows, wrists, hips, knees, ankle joints, ankle-calf joints, tarsal joints and the neck section of the spine. The left and right MCP and PIP joints, on the other hand, are evaluated together in groups, while the temporomandibular, sternoclavicular or acromioclavicular joints undergo collective evaluation.
Depending on their response to pressure, the joints or groups of joints may receive the following scores: 0 – free of pain; 1 – tenderness; 2 – tenderness with wincing 3 – tenderness with wincing and withdrawal. The maximum number of points is 78 [15].
Assessment of joint involvement using certain scales, e.g. the Rheumatoid Arthritis Disease Activity Index (RADAI) or Routine Assessment of Patient Data Index (RAPID-4), may be performed by the patient [14, 16]. On a scale of 0–3, the patient evaluates pain in 16 joints or groups of joints, right and left, respectively: the shoulders, elbows, fingers, hips, knees, ankle joints and toes. The range of points is 0–48.
Laboratory tests are another component for evaluation of the activity of the inflammatory process in the joints – in these circumstances, such inflammatory indicators as CRP or ESR are used.
When joint involvement is observed in patients with systemic CTD, the most commonly used methods of assessment of the activity of the inflammatory process in the joints are the same as those used in RA, and they include: DAS28–ESR, DAS28–CRP, DAS44–ESR, DAS44–CRP, SDAI, CDAI, RAPID-4 as well as the swollen to tender joint count ratio (STR ) index [17, 18] (Table I).
Table I
Recommended indices for assessment of arthritis activity
The disease activity score 28 index is one of the most frequently used scales in rheumatology and it involves examination of 28 joints for swelling and tenderness, the VAS Scale of disease activity completed by the patient as well as ESR or CRP, depending on modification.
The result is obtained by means of a complicated logarithmic pattern; therefore possession of a special calculator is necessary; when the result is < 3.2, the activity of arthritis is low, and when the result is above 5.1, it is estimated as high.
The Clinical Disease Activity Index is concerned with the examination of 28 joints for tenderness and swelling as well as the disease activity assessment both by the patient and physician. It does not, however, contain the laboratory component.
In contrast to the CDAI Scale, the SDAI Scale contains the laboratory component (CRP), which makes the scale more reliable but it takes longer to get the result. The rating system on these scales is simple and it involves adding up all the components [17].
The swollen to tender joint count ratio index is a new and fairly simple tool but its reliability in the assessment of involvement of the peripheral joints is quite high. The swollen to tender joint count ratio index is calculated as a ratio between the number of swollen joints and painful joints (28 joints are assessed; < 0.5 – low activity; > 1 – high activity) [18, 19].
This index appears to show expression of the activity of the inflammatory process in the joints in a more reliable way in comparison to DAS28–ESR since in the commonly used DAS28 index the number of tender joints is twice as important as the number of swollen joints to obtain the final value of DAS28–ESR, whereas, according to practising rheumatologists, a realistic assessment of the inflammatory process in the joints is reflected by the number of swollen joints [20, 21].
Joint tenderness in patients with a long-term course of disease may often be secondary to the advanced degenerative locomotor changes and it does not directly result from the active inflammatory process [22].
Other indices which have gained validation in the assessment of the inflammatory activity in the joints are such scales as patient activity score (PAS), PAS-II, RADAI, or, most frequently used, RAPID-3, thanks to which patients evaluate arthritis activity by themselves.
The RAPID-3 index consists of a Multi-Dimensional Health Assessment Questionnaire form (MDHAQ), which by means of 10 domains evaluates the effect of the disease on everyday life (on a scale of 0–3), and the VAS Scale, in which pain and disease activity are assessed by the patient. After application of the pattern: MDHAQ X 3.33 + VAS of pain + VAS of disease activity/3, the result is obtained on a scale of 0–10: low activity < 2.1; high activity > 4 [23, 24].
The patient activity score and PAS II are very similar to the RAPID-3 index, the only difference being the used HAQ index, i.e. HAQ and HAQ-II, respectively. The Rheumatoid Arthritis Disease Activity Index, on the other hand, is an index consisting of 5 domains: examination of the patient’s joints, duration of morning stiffness, assessment of disease activity during the last 6 months, current assessment of the disease activity and pain severity evaluated by the patient on the VAS Scale.
After calculation, the result is obtained on a scale of 0–10, and a result below 2 is indicative of low disease activity [17].
In the age of the COVID-19 pandemic, having received appropriate training by the physician, the patient-completed scales mentioned above may provide information about the disease activity, especially in the case of telephone consultations. They may also be helpful in making appropriate diagnostic and therapeutic decisions.
Response criteria approved by the American College of Rheumatology (ACR) and Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT), which are commonly used in clinical tests, are a noteworthy way to assess the disease activity. These criteria evaluate 7 components: tenderness and swelling of the joints (28 or more joints can be assessed), acute phase indicators (CRP or ESR), functional capacity scale evaluated by the patient, e.g. HAQ, evaluation of pain by both the patient and physician, most often executed on the 10-degree VAS Scale.
In order to obtain 20%, 50% or 70% improvement, depending on the selected indicator, i.e. ACR20; ACR50 or ACR70, an adequate improvement in the number of joints, both tender and swollen, must be noted. Additionally, improvement in at least 3 out of 5 of the remaining components must be observed [25–27].
Methods of assessment of joint involvement in the course of systemic lupus erythematosus
In order to evaluate the activity of the articular inflammatory process in the course of SLE, the scales determining the general activity of the disease are routinely used, i.e. SLEDAI, Systemic Lupus Erythematosus Activity Measure – Revised (SLAM-R) or European Consensus Lupus Activity Measurement (ECLAM) as well as BILAG-2004, a scale for assessment of the involvement of specific bodily organs in the course of the disease (Table II) [8, 28, 29].
Table II
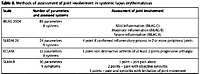
Methods of assessment of joint involvement in systemic lupus erythematosus
The European Consensus Lupus Activity Measurement Scale consists of 12 parameters evaluated during the last 2 weeks. On a scale of 0.5–2, the involvement of a particular organ, severity of a given symptom or abnormality in laboratory tests are evaluated; the maximum number of points is 17.5. When muscle involvement, neuropsychiatric manifestations or haemolytic anaemia is present, another 2 points are added because of the significance of the involvement of a given bodily system.
On this scale, as far as the articular component is concerned, the patient receives only 1 point when it is a non-destructive form of arthritis and when at least 2 peripheral joints are involved (the wrists, MCP or PIP), or in the case of progressive arthralgia manifested as a new pain or deterioration of the localized pain with no inflammatory symptoms in at least 2 peripheral joints [30, 31].
The Systemic Lupus Erythematosus Activity Measure – Revised Scale assesses 30 parameters in a semi-quantitative way (23 clinical signs and 7 laboratory parameters). The maximum value on this scale is 81. The articular component is assessed just like the other parameters and estimated on a scale of 0–3, where 1 = joint pain alone; 2 = pain with objective synovitis; 3 = pain with synovitis and limiting function of the joint [32, 33].
The SLEDAI Scale, on the other hand, in its most frequent form, i.e. SLEDI-2K, evaluates 24 parameters of 9 bodily organs/systems whose involvement is assessed from 1 to 8 points, depending on the clinical significance of the involvement of a given system or severity of a given symptom, and the maximum number of points on this scale is 105. On the SLEDAI-2K Scale, joint involvement is given 4 points when the inflammatory process affects 2 or more peripheral joints [8, 34].
The British Isles Lupus Assessment Group Scale is the most complex scale for evaluating SLE activity. It is an organ-specific scale which consists of as many as 86 parameters, both clinical and laboratory. Some of these parameters, such as laboratory test results, undergo objective evaluation, while the remaining ones are subjectively assessed in comparison to the previous month.
On this scale, the articular domain is divided into 3 categories: mild inflammation/arthralgia/myalgia, moderate inflammation/tendonitis and inflammation of tendon sheaths as well as severe inflammation.
According to this scale, mild inflammation occurs when only arthralgia with morning stiffness is observed, moderate inflammation manifests itself by swelling and tenderness in one or more joints with disturbance of the instrumental functions of everyday life, e.g. doing household jobs was difficult for at least a few days in the previous month.
Severe inflammation is defined by synovitis in two or more joints which significantly disturbs fundamental everyday activities, e.g. dressing. Each articular domain is separately assessed and compared to the assessments from the previous month, and it may be determined as improvement, deterioration, no change or a new organ involvement [8, 35].
However, it must be remembered that each scale has its faults and limitations. For instance, on the SLEDAI Scale, a 6-point increase is regarded as clinically significant and it is indicative of the necessity to intensify therapy, while joint involvement alone is given only 4 points, so if we followed this indication to the letter, we would not have to alter the treatment.
Another downside of this scale is that it does not assess improvement or deterioration in a given category, which means that with the use of this scale alone our assessment will be similar even if the patient presented the involvement of 2 joints a month ago and now he or she presents involvement of 20 joints [8].
Despite its complexity, the BILAG Scale is free of this downside since each of its domains is assessed in comparison to the previously performed assessments and the change is easy to notice. Also, it seems that making therapeutic decisions on the basis of the BILAG Scale is more appropriate because in the case of severe joint involvement (assessed as deterioration or a new involvement) it falls into category A, which is suggestive of high disease activity and thus intensification of therapy is indicated.
When arthritis assumes a moderate form, it falls into category B, which is suggestive of moderate disease activity. Mild joint involvement, however, falls into category C of BILAG and requires only symptomatic treatment [8].
Summing up, on all the scales assessing the inflammatory activity of the joints, regardless of the involvement of 2 joints or more, the scoring system is the same, and if the assessment on the scale was followed to the letter, therapeutic decisions would not always be appropriate.
Thus, it appears that using the BILAG, SLEDAI, ECLAM or SLAM-R Scales alone is unsatisfactory/insufficient, and additional use of general indices, such as DAS28 or the STR index, may be helpful in making proper therapeutic decisions [3].
Methods of assessment of joint involvement in the course of primary Sjögren’s syndrome
The most commonly used scales for assessment of pSS activity include the European Alliance of Associations for Rheumatology (EULAR) Sjögren Syndrome Disease Activity Index (ESSDAI) and the EULAR Sjögren Syndrome Patient-Reported Index (ESSPRI) [36–40]. The ESSDAI Scale consists of 12 domains covering various systems, i.e. constitutional, lymphadenopathic, biological, cutaneous, respiratory, renal, muscular, articular, involvement of the peripheral nervous system and central nervous system, haematological or glandular.
In each of these domains a different number of points is given depending on the significance of involvement of a particular bodily system and the effect on general prognosis and survival. The highest number of points is given in the case of involvement of the muscular and central nervous systems (6 points), the peripheral nervous system, kidneys and lungs (5 points).
A low number of points is given for such domains as: biological (1 point), haematological, glandular and articular (2 points). Next, depending on the degree of involvement, an appropriate multiplier is used regarding the activity: no activity – 0; low activity – 1; moderate – 2; high – 3. It ought to be remembered that when irreversible damage lasting longer than 12 months is observed, it should be assessed as 0 in a given domain.
Similarly to RA, in the case of joint involvement, 28 joints are assessed. The following assessment is used: low activity – when arthralgia is present, e.g. in small joints of the hand, feet with morning stiffness lasting longer than 30 minutes; moderate activity – when synovitis has developed in 1–5 out of 28 joints; high activity – when synovitis has developed in more than 6 joints out of 28.
Thus, in the case of high activity, the maximum number of points is 6 (Table III).
Table III
European Alliance of Associations for Rheumatology Sjögren’s Syndrome Disease Activity Index
An important aspect of the ESSDAI Scale is the fact that moderate activity in pSS occurs when ≥ 5 is obtained, and significant improvement is observed when there is a drop by more than 3 points. Thus, when only the articular domain is taken into account, moderate activity occurs only at the maximum joint involvement, whereas a significant drop occurs when high activity turns into low activity.
Another important scale used for assessment of pSS activity is the ESSPRI Scale. This diagnostic tool is intended for patients to carry out self-assessment of the disease. It consists of 3 numerical scales (0–10) in which 3 pSS features are assessed every 2 weeks, i.e. dryness (the patient is to evaluate dryness of the eyes, mouth as well as global dryness), fatigue as well as pain in the joints or muscles of the lower limbs.
An international study including 395 patients showed that the mean assessment on the ESSPRI Scale is 6; dryness was the most significant aspect of the disease in 45.4% of the patients, fatigue in 36.5%, and pain in 18.1% [36]. It can be surmised that, with all the complexity of the disease, on the basis of the ESSPRI Scale every fifth patient presents clinically significant joint involvement, which is contradictory to the ESSDAI Scale, where the articular aspect is not such a significant component of the disease.
The same study also revealed that the ESSDAI Scale evaluating the involvement of internal organs and the ESSPRI Scale determining patient-reported symptoms showed no correlation with one another. This means that these two maximal aspects of the disease do not overlap, and in order to carry out appropriate and complete assessment of pSS activity, including of patient-reported symptoms, both of these scales should be used [36].
Moreover, similarly to SLE, investigations demonstrate that using the DAS28 Scale (ESR) as well as DAS28–CRP has adequate sensitivity in the assessment of pSS activity. What is more, these indicators show a good correlation with the articular domain of the ESSDAI Scale [41].
Summing up, it seems advisable that in order to demonstrate joint involvement in pSS thoroughly, the diagnostic tools employed in pSS, i.e. ESSDAI and ESSPRI, should be used in connection with the DAS28 Scale. Thanks to this the treatment of patients suffering from pSS will be more comprehensive and complete.
Methods of assessment of joint involvement in the course of systemic sclerosis
An important matter in SSc is determining whether the disease is in the active phase or if irreversible organ changes have already occurred. Distinguishing between these two phases, often changing smoothly from one into the other, is vital since the active phase is connected with the inflammatory process, it is reversible and therefore launching intensive immune-suppressive therapy may stop the course of the disease and prevent organ damage [42].
One of the most important diagnostic tools for the assessment of the active phase of systemic scleroderma is the SSc activity index developed by the European Scleroderma Research Group Activity Index (EscSG-AI) [43].
This tool consists of 10 components divided into clinical signs and accessory investigations, each of which is given 0.5–2 points. The maximum number of points on this scale is 10, and the active phase of the disease is assumed when the activity index is > 3.
On this scale, the articular domain has only 0.5 points, which indicates that in the opinion of the authors of the scale the joint involvement is not of the utmost importance and it should not have a major influence on therapeutic decisions.
In response to criticism that the EscSG-AI Scale did not objectively assess the right SSc severity, the European Scleroderma Trials and Research Group (EUSTAR) developed the Activity Index (EUSTAR-AI) (Table IV) [44].
Table IV
European Scleroderma Trials and Research Group Activity Index
This tool consists of only 6 components, i.e. severity of skin lesions assessed by the patient, ulceration of finger tips, modified indicator of Rodnan skin involvement (modified Rodnan skin score – mRss), CRP, diffusing capacity for carbon monoxide, and tendon friction. This scale does not contain the articular component since in the researchers’ opinion it was insignificant as a prognostic factor.
On the other hand, it should be noted that tendon friction and elevated CRP, often connected with arthritis, are given the highest score, i.e. 2.25 points. This is because both tendon friction and arthritis are predictors of SSc progression, and they correlate with organ involvement progression [45].
It has been observed that a group of patients with tendon friction presented generalized skin involvement, higher disease activity, and they were more frequently diagnosed with disability.
Moreover, in this group of patients, a 3–5-fold increased risk of development of scleroderma renal crisis, CVS involvement (lowering of the ejection fraction), digestive tract involvement as well as ulceration of finger tips or gangrene was observed [45].
Functional assessment in SSc may be carried out using such tools as the Hand Mobility in Systemic Scleroderma Scale (HAMIS) [46], Modified HAMIS Scale (mHAMIS), Cochin Hand Function Scale or the HAQ Scale [47].
For example, the HAMIS Scale evaluates 9 types of hand movements such as bending and straightening of fingers, thumb abduction, tweezers grip, finger abduction, dorsal extension of the hand, palmar flexion, pronation and supination. Each component is evaluated on a scale of 0–3, where 0 means normal mobility, whereas 3 means total inability to perform a certain movement. The maximum number of points is 27 and achieving this number means complete hand dysfunction. Easier to use, and still with adequate sensitivity and reliability, is the mHAMIS Scale, which investigates only bending and straightening of fingers, finger abduction and dorsal extension of the hand [48].
In contrast to RA, in SSc, limitation of functional capacity of the hand is connected not only with inflammatory activity of the joints or joint destruction but also with hardening of the skin, ulcerations, self-amputation of phalanges or tendon friction.
Therefore, the use of this tool does not fully demonstrate the musculoskeletal involvement in the disease. It is significant that as many as 90% of SSc patients presented hand mobility limitation, which had a negative effect on performing everyday activities [49].
Correct and early determination of the extent of hand disability in this group of patients may be helpful in selecting an appropriate rehabilitation programme and prescribing proper pharmacological treatment before complete contractures develop and hand functionality is completely lost [50].
Therefore, in contrast to the BILAG Scale, the scales for assessment of SSc activity, e.g. EscSG-AI or EUSTAR-AI, provide incomplete assessment of the severity of the locomotor system involvement. The scales assessing functionality, on the other hand, determine the degree of organ damage, which is dependent on both the musculoskeletal system and skin involvement, rather than the inflammatory activity in the joints.
Thus, it seems that in order to determine the severity of the locomotor system involvement more objectively, the scales for the assessment of pSS activity, i.e. SDAI, CDAI, DAS28–CRP or DAS28–ESR, that are also reliable in the assessment of arthritis in the course of SSc, should be used [51, 52].
Discussion
Joint involvement in the course of systemic CTD is usually milder than in RA. Most often it is manifested by pain in the locomotor system, but poly-arthritis or even destructive arthritis may develop.
Therefore, joint changes in systemic CTD constitute a significant clinical problem since in many patients they can reduce their quality of life and lead to functional limitations or, in extreme cases, to disability; they can also worsen the prognosis of the disease. That is why appropriate assessment of joint involvement in the course of CTD is a great diagnostic challenge for specialists concerned with the locomotor system.
Due to the multi-systemic nature of diseases, it is difficult to find the right tools for the assessment of CTD activity; in many cases the involvement of the locomotor system overlaps with symptoms from other internal organs as well as with general symptoms, which may significantly affect the assessment of the locomotor system.
The use of scales intended for the assessment of particular CTD in combination with the scales for the assessment of RA seems to be the best solution because the articular aspect is often only one of the components on the CTD assessment scale and it does not show any difference in the number of the affected joints like in the SLEDAI Scale, for example.
In addition, in the age of the COVID-19 pandemic, using the patient-completed scales, e.g. RAPDI-3, RADAI together with the subjective arthritis assessment, HAQ, the VAS Scale or the ESSPRI in the assessment of pSS, appears to be a helpful solution [53].
Regular use of scales assessing the locomotor system in the course of CTD allows for more precise assessment of arthritis activity, enables determination of improvement or deterioration, and therefore is helpful in making timely diagnostic and therapeutic decisions.
Conclusions
Joint involvement is one of the most common clinical manifestations of systemic CTD.
In the course of CTD, joint symptoms may be one of the domains suggesting a severe course of the disease involving multiple internal organs.
The search for appropriate scales to determine the degree of joint involvement is very important in assessing the severity of joint changes and helps for timely implementation of appropriate treatment.
The use of scales intended for the assessment of particular CTD in combination with the scales for the assessment of RA seems to be the best solution.