
Introduction
Rheumatoid arthritis (RA) is a key disease in the field of rheumatology. Since the 1990s, the understanding of RA has changed significantly thanks to advances in the knowledge of its natural history and key pathogenic mechanisms. Consequently, treatment strategies have evolved accordingly and continue to do so. In the 1980s, it was common clinical practice to delay the initiation of disease-modifying antirheumatic drugs (DMARDs) until later stages of the disease due to concerns about adverse effects and toxicity. However, this approach was quickly abandoned after early joint destruction was observed even during the initial stages of the disease [1–3].
Methotrexate (MTX) was introduced nearly 50 years ago as an effective agent for autoimmune inflammatory polyarthritis and was approved by the U.S. Food and Drug Administration in 1987 as first-line therapy for RA. Before the turn of the millennium, a wide range of potent biological agents emerged as effective therapeutic options for patients with RA who did not respond to MTX or other conventional synthetic DMARDs [4].
The list of biological agents approved for RA is extensive and includes abatacept, tocilizumab, anakinra, etanercept, and infliximab, among others. One molecule that has drawn special attention because of its mechanism of action and broad indications in rheumatologic diseases – many still considered off-label – is rituximab (RTX) [5].
Rituximab is a chimeric monoclonal antibody directed against the CD20 antigen expressed on B lymphocytes. This antigen is present on pre-B and mature B cells, and RTX acts by depleting this critical cell lineage, leading to inactivation and apoptosis and thereby eliminating entire populations of autoreactive B cells [6, 7].
The 2022 European Alliance of Associations for Rheumatology (EULAR) consensus on RA included 11 recommendations for the evaluation and management of the disease, emphasizing that all biological agents (and targeted synthetic agents such as tofacitinib) should ideally be administered in combination with a conventional synthetic DMARD such as MTX to enhance efficacy, improve adherence, and reduce the development of anti-drug antibodies [8].
However, biological monotherapy may be necessary in various clinical scenarios, including adverse reactions, intolerance, toxicity, specific medical indications, or sustained remission [9, 10].
An increasing body of literature supports the use of biological monotherapy, suggesting that there may be no substantial difference in outcomes compared with combination therapy, despite current EULAR and American College of Rheumatology (ACR) guidelines favoring the latter. Although results vary, the overall trend indicates that monotherapy may be equally – or even more – effective in patients with RA refractory to conventional treatment [11, 12].
At our referral center, we treat patients with RA using RTX in combination with conventional synthetic DMARDs: MTX, leflunomide (LFN), sulfasalazine, azathioprine, hydroxychloroquine, as well as a subgroup who receive RTX monotherapy for various reasons (intolerance, prior DMARD toxicity, contraindications, physician recommendation, or patient preference). In this context, we designed a study to determine the efficacy of RTX monotherapy in patients with RA refractory to standard therapy.
The main objective was to evaluate the efficacy, safety profile, and treatment adherence of RTX monotherapy compared with combination therapy with MTX or LFN in patients with RA treated at our institution.
Material and methods
Study population
Patients diagnosed with RA according to the 1987 ACR or 2010 ACR/EULAR classification criteria who were receiving RTX as monotherapy or in combination with MTX or LFN were included. A total of 157 patients were enrolled and classified into 3 groups: group 1 – RTX monotherapy (n = 48), group 2 – RTX + MTX (n = 66), group 3 – RTX + LFN (n = 43).
Group allocation was based on prior treatment history and clinical criteria. RTX monotherapy: patients with documented intolerance to MTX or LFN, hepatic or renal disease, or those who refused MTX or LFN; RTX + MTX: patients already receiving MTX prior to starting RTX; RTX + LFN: patients already receiving LFN prior to adding RTX. All patients had previously failed conventional therapy (MTX or LFN for at least 3 months) and subsequently failed biologic therapy with 2 anti-tumor necrosis factor (TNF) agents (etanercept, infliximab, or adalimumab for at least 6 months each), for which RTX was indicated as a third-line biologic.
Patients were followed for 12 months and evaluated at weeks 1, 24, and 48 using the following disease activity indices: Health Assessment Questionnaire (HAQ), Disease Activity Score in 28 joints (DAS28), American College of Rheumatology 70% response (ACR70; 70% improvement in tender/swollen joint counts according to ACR criteria), Treat-to-Target (T2T) – defined as ≥ 50% reduction in DAS28 at 3 months and remission or low disease activity (DAS28 < 3.2) at 6 months.
All patients received premedication with 100 mg of methylprednisolone (as per RTX product information). Dosage: RTX 1 g IV on days 1 and 15 every 6 months; MTX 10–15 mg orally once weekly; LFN 20 mg orally once daily. Patients receiving 2 or more conventional DMARDs were excluded. All patients initiated treatment with medium-dose glucocorticosteroids (GC; equivalent to 7.5–30 mg of prednisone daily).
Exclusion criteria: pregnancy, chronic kidney disease, heart failure, seronegative RA, and coexistence of other autoimmune diseases.
Interpretation of disease activity scores: HAQ: 0 = no difficulty; 1 = mild to moderate; 2 = severe difficulty; 3 = inability to perform tasks. DAS28: < 2.6 = remission; 2.6–3.2 = low activity; 3.2–5.1 = moderate activity; > 5.1 = high activity. ACR70: based on joint counts, functional capacity, pain assessment, and inflammatory markers.
Classification of adverse events: mild – headache, myalgia, dyspepsia, low-grade fever; moderate – urinary tract infections, respiratory infections, localized herpes zoster, elevation of liver enzymes > 2×, urticaria, tachycardia; severe – tuberculosis, sepsis, anaphylaxis, drug-induced lupus, vasculitis, pancytopenia, lymphoma, malignant neoplasm, hypotension, bronchospasm, seizures.
Treatment adherence was assessed using a mixed strategy depending on medication type: for RTX, the percentage of doses administered vs. prescribed doses over the 12-month follow-up; for MTX and LFN, prescription and dispensing records were reviewed through the electronic medical record and complemented by direct patient interviews during quarterly visits, using the Morisky-Green-Levine questionnaire (“Have you ever forgotten to take your medication in the last few days?”). A patient was considered adherent if they reported regular compliance and medical records confirmed continuous drug withdrawal (refill) throughout the follow-up period.
Refractory RA was defined as persistent moderate-to-high disease activity despite adequate use of at least 2 conventional synthetic DMARDs (such as MTX or LFN) for a minimum of 3 months, and failure or loss of efficacy with 2 anti-TNF biologic agents, each administered for at least 6 months. This definition follows the EULAR 2022 recommendations for the management of difficult-to-treat RA.
Study variables
Independent variable: treatment type (RTX, RTX + MTX, RTX + LFN). Dependent variables: disease activity scores (HAQ, DAS28, ACR70, T2T). Control variables: age, sex, disease duration, GC use. Safety variable: adverse events.
Although EULAR/ACR response criteria are widely used in clinical trials, they were not applied in this study because local clinical records did not include all required parameters (e.g., simultaneous physician and patient global assessments). Therefore, quantifiable and consistently available indicators in the cohort (DAS28, HAQ, ACR70, and T2T) were prioritized. The T2T approach was applied retrospectively by reviewing clinical charts and serial DAS28 values at weeks 12, 24, and 48. A response was considered adequate when patients achieved a ≥ 50% reduction in DAS28 at 3 months and remission or low disease activity (DAS28 < 3.2) at 6 months, in accordance with international recommendations. This procedure allowed for consistent evaluation of treatment goal adherence across all groups.
Statistical analysis
ANOVA was used for continuous quantitative variables (DAS28 and HAQ), while c2 tests were applied to ordinal categorical data (ACR70 and T2T criteria). Multivariate analysis included linear regression for DAS28 and binary logistic regression for ACR70. Results were presented in tables and profile graphs using IBM SPSS Statistics v25.
Results
Clinical and epidemiological characteristics
A total of 157 patients were evaluated. The mean age in each group was as follows: RTX monotherapy – 52.4 years; RTX + MTX – 46.6 years; RTX + LFN – 56.7 years. Females predominated across all groups (only 9 males in the entire cohort). The mean disease duration was longer in the RTX + MTX group (3.5 years) compared with the RTX monotherapy group (2.7 years) and the RTX + LFN group (2.1 years). A total of 28 adverse events were recorded in the RTX + LFN group, compared with 14 in the RTX monotherapy group and 16 in the RTX + MTX group. None of the patients discontinued treatment due to adverse reactions.
Comparison of treatment efficacy among groups
The efficacy results for the three treatment groups are summarized in Table I. The efficacy of the 3 therapeutic regimens (RTX monotherapy, RTX + MTX, and RTX + LFN) was evaluated. All groups showed progressive clinical improvement throughout the 12-month follow-up period. At week 48, mean HAQ scores were 1.7 (RTX monotherapy), 1.1 (RTX + MTX), and 1.8 (RTX + LFN). This reduction was statistically significant in all 3 groups (p < 0.005, ANOVA). Similarly, DAS28 scores decreased from baseline values of 5.8, 5.6, and 5.7, respectively, to 1.3, 1.6, and 1.6 at week 48. These changes were also statistically significant (p < 0.005, ANOVA).
Table I
Comparison of treatment efficacies in the 3 study groups
Regarding the ACR70 response criterion, there was a progressive increase in the proportion of patients achieving this clinical response. At week 48, 82% of patients in the RTX monotherapy group achieved ACR70, compared with 85% in the RTX + MTX group and 80% in the RTX + LFN group (p < 0.005, c2 test).
Finally, the T2T criteria were applied to evaluate clinical outcomes. A response was considered adequate if patients achieved a 50% reduction in DAS28 at 3 months (week 12) and remission or low disease activity (DAS28 < 3.2) at 6 months (week 24). Only the RTX monotherapy group did not meet the 3-month T2T criteria; the remaining groups achieved all proposed T2T goals.
To minimize potential confounding from baseline differences in age, disease duration, and initial DAS28 scores, stratified analyses and adjusted models were performed.
In the multivariate linear regression model (dependent variable: DAS28 at week 48), treatment type (RTX alone, RTX + MTX, or RTX + LFN) remained an independent predictor of disease activity reduction after adjustment for baseline DAS28, age, and disease duration (p = 0.004). Similarly, in the binary logistic regression model (dependent variable: achievement of ACR70 at week 48), the use of RTX monotherapy showed a favorable trend (adjusted OR = 1.48; 95% CI: 0.89–2.46), although not statistically significant (p = 0.11). Stratified analyses by baseline DAS28 tertiles confirmed consistent results across subgroups, with no significant interaction between initial disease activity and therapeutic response.
Comparison of adverse events among groups
The distribution of adverse events across the three groups is presented in Table II. During the 12-month follow-up, 53 adverse events were recorded. Mild events (n = 27; 50.9%) included headache, myalgia, and dyspepsia. Moderate events (n = 21; 39.6%) were mainly respiratory or urinary tract infections, localized herpes zoster, and transient elevation of liver transaminases. Severe events (n = 5; 9.4%) included hypotension (n = 2), bronchospasm (n = 1), seizures (n = 1), and urinary sepsis (n = 1). No deaths or treatment discontinuations due to adverse events were reported. Comparative analysis among groups revealed no statistically significant differences in the frequency or severity distribution of adverse events (p > 0.05, χ2 test).
Comparison of treatment adherence among groups
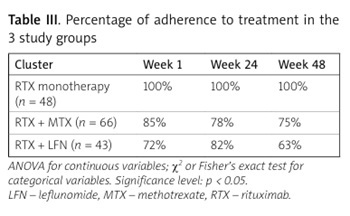
Treatment adherence rates at weeks 1, 24, and 48 are shown in Table III. Significant differences in treatment adherence were observed (week 1: p = 0.0098; week 24: p = 0.0006; week 48: p = 0.00004). The RTX monotherapy group showed 100% adherence at all time points, whereas the combination therapy groups had slightly lower adherence rates. However, it should be noted that hospital-based intravenous administration of RTX ensures directly observed compliance, unlike oral DMARDs (MTX or LFN), whose adherence depends on self-administration at home. Therefore, the observed differences likely reflect the route and mode of administration rather than an intrinsic advantage of monotherapy.
Discussion
This prospective observational cohort study comparing RTX monotherapy with its combination with MTX or LFN in patients with RA is the first of its kind in the region. To date, no previous studies on this topic have been published in Peru.
Rituximab, MTX, and LFN are widely accepted and used treatments for RA worldwide, either as monotherapy or in combination. Each drug has a specific mechanism of action, which may offer a strategic advantage in achieving disease remission or low disease activity, provided that dosage is appropriately prescribed. In our study, all patients receiving MTX were treated with 10–15 mg orally per week, reflecting our local clinical practice and the observed tolerance profile in the Latin American population. We acknowledge that this oral dose (10–15 mg/week) is lower than internationally recommended doses (25–30 mg/week subcutaneous), which may have influenced the comparability of the results.
Our study found no statistically significant differences in efficacy among the 3 treatment groups (RTX monotherapy, RTX + MTX, and RTX + LFN), confirming that all regimens can achieve disease remission in patients with RA. Furthermore, no correlation was found between clinical improvement and rheumatoid factor levels, frequency of adverse events, or prednisone dosage. Treatment adherence was higher in the RTX monotherapy group. However, this difference should be interpreted with caution, as RTX infusions are administered in a hospital setting under direct supervision, whereas adherence to oral DMARDs in combination regimens depends on patient self-administration. Therefore, the higher adherence observed in the monotherapy group likely reflects the route of administration and clinical supervision rather than a true behavioral difference in treatment compliance.
In addition, our study did not apply the EULAR/ACR response criteria decision based on the partial availability of clinical parameters in local records. Instead, we employ validated and complete quantitative measures from our database (DAS28, HAQ, ACR70, and T2T), ensuring objective follow-up. The retrospective application of the T2T approach, based on serial DAS28 values, ensured consistency in the evaluation of clinical response, although we recognize that this retrospective nature may introduce an inherent information bias.
Our conclusions are consistent with most previous studies. Wang et al. [13] published a meta-analysis assessing the efficacy and safety of RTX combined with MTX vs. MTX alone in RA patients, finding that RTX + MTX was more effective in achieving remission, while infection and complication rates were similar between groups. Koehm et al. [14] conducted a randomized clinical trial comparing RTX + LFN with placebo + LFN, reporting higher remission rates in the RTX + LFN group and recommending an initial RTX dose of 1,000 mg. A similar study confirmed that RTX + LFN is effective in achieving remission or low disease activity but was associated with severe adverse events such as systemic infections and musculoskeletal disorders [15].
Sebastiani et al. [16] compared RTX monotherapy and RTX + MTX combination therapy in a 104-week follow-up study. Both groups achieved remission, and the number of adverse events was comparable. The authors concluded that remission can be achieved with either RTX monotherapy or RTX + MTX combination therapy. Richter et al. [17] performed a retrospective study comparing RTX, MTX, and LFN in RA patients over a 6-year period. Their cohort included 294 patients on RTX monotherapy, 496 on RTX + MTX, and 117 on RTX + LFN. The lowest prednisone doses were observed in the RTX + LFN group. Although adherence was lower in the RTX monotherapy group, all 3 regimens appeared equally effective in achieving remission [17].
Edwards et al. [18] conducted a similar study in RA patients, assigning 4 treatment groups: MTX monotherapy, RTX monotherapy, RTX + MTX, and RTX + cyclophosphamide. After 48 weeks, no significant differences were found in achieving ACR50 or ACR70 scores. Most adverse events were reported in the RTX monotherapy group [18]. Chatzidionysiou et al. [19] published a large European observational cohort study with 3 groups: RTX monotherapy (n = 505), RTX + MTX (n = 1,195), and RTX + LFN (n = 177). After 1 year, the RTX + LFN group showed the highest remission rate (29.1%) compared with RTX monotherapy (19.3%) and RTX + MTX (21.1%). Adverse event rates were similar among groups [19].
Raiter et al. [20] conducted a similar study in Israeli RA patients comparing RTX monotherapy, RTX + MTX, and RTX + LFN. No significant differences were found in biological survival or discontinuation rates. The authors emphasized the need for further studies to assess the long-term sustainability of RTX monotherapy. Likewise, registry studies and international reviews have provided additional evidence regarding RTX monotherapy vs. combination therapy.
Cohen et al. [21] performed a systematic review of major clinical trials and registry data, concluding that RTX monotherapy maintains sustained clinical efficacy and a comparable safety profile to combination regimens with MTX or LFN, particularly in patients with intolerance or contraindications to conventional synthetic DMARDs. Consistently, Łosińska et al. [22] published a multicenter observational registry-based study conducted in real-world clinical practice, demonstrating that long-term efficacy and treatment survival of RTX are equivalent between monotherapy and combination regimens, with no significant increase in serious adverse events.
In our study, adverse events did not differ significantly between groups, consistent with the findings of Shi et al. [23], who performed a meta-analysis of RTX-related infections in RA. They analyzed 11 studies involving 9,502 RA patients and concluded that the overall infection rate was similar between RTX users and non-users.
Study limitations
Our study has several limitations. It was a single-center study with data collection performed by a single investigator, introducing potential selection bias, information bias, and Berkson’s bias. The inclusion of patients in the monotherapy group (due to intolerance or refusal of MTX or LFN) may have affected baseline comparability among groups. Another relevant limitation is the small number of severe adverse events recorded, which restricts statistical power for definitive safety comparisons. Although no significant differences were observed, this low event count prevents excluding potentially relevant clinical variations.
In addition, serial immunoglobulin measurements (IgG, IgA, IgM) were not performed – a key parameter for monitoring RTX safety, particularly regarding the risk of hypogammaglobulinemia or recurrent infections. The absence of these data represents an important limitation that should be addressed in future studies.
Conclusions
Rituximab monotherapy is as effective and safe as combination therapy with MTX or LFN in patients with RA. Although no significant differences in the frequency of adverse events were observed, the limited number of severe cases and the lack of immunoglobulin assessment limit the interpretation of the safety findings.
Future studies should include systematic immunological monitoring and larger sample sizes to confirm these results. Our findings should be interpreted with caution due to the single-center design, limited sample size, lower MTX dose, and potential selection bias. Therefore, while the results suggest comparable efficacy and safety, they do not establish clinical equivalence between the evaluated regimens.