
Introduction
Systemic sclerosis (SSc) is an autoimmune systemic disease characterized by multisystem organ involvement. Clinical features of SSc are are thought to result from endothelial injury in the microcirculation that results in fibrosis of the skin and visceral organs [1]. Nailfold video capillaroscopy (NVC) is proposed as a non-invasive tool for the assessment of microvascular abnormalities. Clinical features of vascular involvement in SSc including Raynaud’s phenomenon (RP), digital pitting scar, gangrene, scleroderma renal crisis, and primary pulmonary hypertension (PH). Additionally, the primary cause of SSc-related primary heart involvement (SSc-pHI) is is believed to be microvascular system impairment [2].
Systemic sclerosis-related primary heart involvement was first defined in 2001. It is diagnosed when the patient presents with myocardial disease (myocarditis, myocardial fibrosis), heart failure, conduction system abnormalities, and pericardial disease, after ruling out secondary causes of cardiac involvement [3].
Studies investigating NVC features and SSc-pHI are scarce. Some studies have referred to the association between NVC abnormality, coronary microcirculatory dysfunction, and left ventricular dysfunction [1, 4]. Altered vasoactivity in the cardiac microcirculation may cause focal ischemic injury and fibrotic lesions. Ischemia in the cardiac microcirculation and subsequent fibrosis may result in arrhythmias, conduction blocks, or other electrocardiographic abnormalities in patients with SSc [5, 6].
Investigating the correlation between microvascular involvement assessed by capillaroscopy and cardiac arrhythmias or conduction blocks may help elucidate aspects of the pathophysiology of SSc-pHI. To our knowledge, no study has assessed microvascular function evaluated by NVC in relation to arrhythmias or conduction blocks. In this novel study, we focused on conductive system involvement, 1 manifestation of SSc-pHI, and assessed the correlation between arrhythmias and conduction blocks and nailfold capillaroscopic staging systems.
Material and methods
Study population
Data from 110 scleroderma patients in this cross-sectional study were extracted from the database of the scleroderma cohort established in 2008. Patients who fulfilled the 2013 American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR) classification criteria for SSc had undergone capillaroscopic examination were included in the study [7]. For this study, demographic data, clinical signs and symptoms, medication history, and laboratory and paraclinical data (routine blood, urine, autoantibodies test, serum pro-B-type natriuretic peptide [pro-BNP] level, and capillaroscopic examination results) were extracted from registry records. We compared the NVC features between the 2 groups of patients.
Study group
One hundred ten patients with SSc underwent an NVC study. The patients were classified into 2 groups based on NVC findings. Thirty-one patients with the cardiac outcome of arrhythmias or conduction block due to SSc-pHI were included in the outcome group. Systemic sclerosis-related primary heart involvement was diagnosed according to the criteria established by the World Scleroderma Association/Heart Failure Association [3, 8].
The group without the outcome consisted of 79 patients. These patients had no cardiac involvement, and if they had arrhythmia or conduction block, they were attributed to pulmonary arterial or systemic hypertension and ischemic heart disease.
The primary cardiac outcome in the study referred to cardiac arrhythmias that needed treatment and were diagnosed by 12-lead electrocardiogram (ECG) trace, or 24-hour Holter monitoring, and cardiac block as high-degree atrioventricular (AV) block or bundle branch block (left bundle branch block [LBBB], right bundle branch block [RBBB]). Cardiac single photon emission computed tomography (SPECT) was performed in patients with LBBB to exclude coronary ischemia. We considered peak tricuspid regurgitation velocity > 3.4 (m/s) was considered a surrogate marker for diagnosing PH [9].
Systemic hypertension, coronary artery disease (history of angina and ECG changes, and cardiac SPECT abnormality in favor of coronary ischemia), and severe valvular heart disease were excluded.
Nailfold video capillaroscopy assessments were performed using a video capillaroscope (Optilia Instruments AB, Sollentuna, Sweden), and images with a 200× magnification were used for analysis. The qualitative, semi-quantitative, and quantitative assessments were defined according to the criteria of the EULAR Study Group on Microcirculation in Rheumatic Diseases [10].
Nailfold video capillaroscopy was performed by 2 examiners (L.A., N.M.) in all patients without knowledge of the study protocol. The examiner inspected the nailfolds of 4 fingers on each hand (1 mm in the medial and lateral of each nailfold), and 2 images were taken and saved for each finger.
Capillary parameters were studied using qualitative and semi-quantitative methods. Reports of the capillaroscopy study review were made by 2 investigators (M.M, M.S.), and in cases of disagreement, a second review was performed to reach a consensus.
The NVC scleroderma pattern classified images as late, active, early, non-specific, or normal [11]. In the semi-quantitative assessment, we used a rating scale to score the NVC parameter changes from 0 to 3 (0: normal, 1: < 30% change, 2: 33–66%, 3: > 33% changes in parameters). Six NVC parameters – capillary loss, enlarged capillaries, giant capillaries, ramified capillaries, disorganized capillaries, and microhemorrhages – were determined according to previous studies [10–14]. In the semi-quantitative scoring system, higher scores indicate more severe alterations. Capillaroscopic parameters were precisely defined to minimize interobserver bias:
capillary loss, the number of capillary loops in the distal row below the normal range [11–15];
enlarged capillaries with an increase in capillary diameter > 20 μm;
giant capillaries, homogenously enlarged loops with a diameter > 50 μm;
microhemorrhages (presence of hemosiderin deposit due to capillary injury);
capillary ramifications: branching, coiled, or bushy-featured capillaries derived from a single normal-sized capillary;
capillary disorganization: capillary with irregular distribution and orientation.
Statistical analysis
For descriptive statistics, numerical data with normal distribution were presented as means ± standard deviation (SD); otherwise they were presented as medians and ranges. The means of the 2 independent groups were compared using Student’s t-test. For variables with non-normal distribution, the median of the 2 groups was assessed using the Mann-Whitney U test. For comparison, the odds ratio (OR) for qualitative parameters on NVC in the 2 study groups was calculated using MedCalc’s calculator. Sensitivity (Se), specificity (Sp), positive predictive value (PPV), and negative predictive value (NPV), as well as the likelihood ratio (LR) of abnormal capillaroscopic parameters for the diagnosis of cardiac outcomes, were computed.
Results
The mean age ±SD of patients in the study was 49.50 ±13.27 years, with no significant those patients with and those without cardiac involvement. The study included 108 (89.3%) female patients. Disease subtypes among patients with cardiac outcomes were as follows: sine scleroderma – 5 (13%), limited cutaneous SSc – 12 (33%), diffuse cutaneous SSc – 19 (52.8%). Esophageal symptoms and RP were seen in 107 (88.4%) and 108 (89%) patients, with no significant difference between the 2 groups.
Telangiectasia and digital ulcer showed no significant difference in the 2 groups (p = 0.81 and p = 0.51, respectively), and pulmonary arterial hypertension (PAH) was present only in 7 patients in the cardiac outcome group. Heart failure (defined by ejection fraction < 50%) was seen only in 3 patients with cardiac outcomes.
Detailed evaluation in these patients indicated cardiomyopathy related to primary heart involvement due to scleroderma. Four patients (3.3%) had scleroderma renal crises (Table I). In our study, diabetes was present in 1 patient within the group of patients without cardiac outcomes. Eight patients (6.6%) were smokers, and 2 of the patients had cardiac outcomes. Serum pro-BNP levels were assessed in 76 (62.8%). Abnormal pro-BNP levels higher than 125 pg/ml were present in 17 (60%) patients with cardiac outcomes and 11 (39%) patients without; the difference was not significant (p = 0.27). Sixty-five patients had received cytotoxic drugs (mycophenolate mofetil or cyclophosphamide) within 6 months prior the capillaroscopy examination, 47 (73%) had arrhythmias or conduction blocks, and 18 (27%) were in the group without.
Table I
Demographic and baseline data in the 2 study groups
Cardiac features in the study
Axis deviation was observed in 15 patients with cardiac disease outcome; 10 had a right axis and 5 had a left axis deviation. Two patients without a cardiac outcome had axis deviation, 1 with left axis deviation and 1 with right axis deviation.
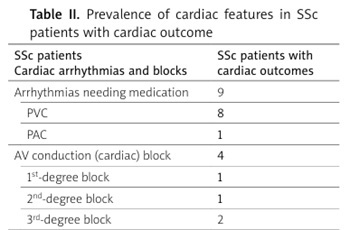
Arrhythmia that requiring treatment was present only in 9 patients with cardiac outcomes. Premature ventricular contractions were more frequent than PACs. Atrioventricular conduction block was seen in 4 patients with cardiac outcomes; 2 patients had complete bundle branch block. A bundle branch block was seen in 23 patients; 7 had complete RBBB, and 4 had complete LBBB (Table II).
Table II
Prevalence of cardiac features in SSc patients with cardiac outcome
Capillaroscopic parameters in the study
Analysis was performed based on conduction block, bundle branch block, ventricular arrhythmias, and atrial arrhythmias (data are not shown). Regarding qualitative NVC analysis, the ORs of early pattern in groups of patients with and those without cardiac outcomes were 0.93 (95% CI: 0.35–2.45; p = 0.89). The ORs of active and late patterns in the 2 groups of patients were 0.92 (95% CI: 0.37–2.30; p = 0.86) and 1.07 (95% CI: 0.52–2.19; p = 0.84), respectively (Table III).
Table III
Qualitative NVC features in SSc patients in the 2 study groups
Comparison of NVC findings according to the presence of cardiac outcomes showed that the mean capillary density score was higher in patients with cardiac outcomes than in those without cardiac outcomes (2.19 ±0.910 vs 1.72 ±1.120, respectively; p = 0.04; a higher capillary density score means greater percentage of capillary loss). Moreover, a comparison of capillaroscopy disorganization showed a mean score ±SD of 1.00 ±0.01 in patients with cardiac outcomes and 0.95 ±0.22 in the group without cardiac outcomes (p = 0. 001). Other capillaroscopy parameters showed no significant differences (Table IV).
Table IV
Nailfold video capillaroscopy characteristics and comparisons between groups of patients with and without cardiac involvement
Diagnostic value of abnormal capillaroscopy parameters for the diagnosis of cardiac outcomes
Low density in the capillary examination was positive in 93 patients (30 with cardiac outcomes, and 63 without). Normal capillary density was observed in 17 patients (1 with a cardiac outcomes, and 16 without). The Se of the test was 96.7%, and the Sp was 18.9%. The PPV was 32%, and the NPV was 94.1%. The positive (LR+) and negative likelihood ratios (LR–) were 1.19 and 0.17, respectively.
Disorganized capillaries in capillary examination were positive in 105 positives out of 110 patients (30 having cardiac outcomes, and 75 without cardiac outcomes), and normal organization in capillaroscopy was present in 5 patients (1 with a cardiac outcome, 4 without cardiac outcomes); test Se was 96.7%, test Sp was 5%, test PPV was 85%, and test NPV was 80%. The LR+ and LR– were 1.12 and 0.66, respectively.
Discussion
In the capillaroscopic study of 121 scleroderma patients, 110 had specific scleroderma patterns. Cardiac arrhythmias and block due to primary cardiac involvement were present in 39 patients. Arrhythmia requiring block was detected in 9 patients, with different degrees of AV block in 4 patients, and bundle branch block in 23 patients (complete RBBB and LBBB in 7 and 4 patients, respectively). There were no associations between qualitative capillaroscopy features (early, active, late) and cardiac outcome. However, the study of semi-quantitative capillary parameters showed decreased density and higher capillarity disorganization in patients with cardiac outcomes. Low-density nailfold and disorganized capillaries in capillary examination implied high sensitivity for the screening of patients for cardiac outcomes.
Primary heart involvement in SSc may be subclinical and detected through clinical investigation. In addition, cardiac condition associated to PAH, renal involvement, interstitial lung disease, hypertension, drug toxicity, valvular disease, and ischemic heart disease must be excluded [3].
There have been no previous studies addressing features of capillary microcirculation on NVC and arrhythmia or block associated with SSc-pHI. However, some studies referred to capillaroscopy features and microvascular involvement of the disease. One study found that a higher avascular score correlated with lower coronary reserve and more coronary microvascular dysfunction [1, 6].
One systematic review indicated that a study on non-invasive capillaroscopy in cardiovascular disease showed increased capillary density and diameter in patients with PAH. Additionally, in the subgroup of patients with SSc, advanced scleroderma patterns in NVC preceded development of PAH [15].
In 1 case-control study, capillary enlargement and hemorrhages in NVC were found more common in scleroderma patients with preserved ejection fraction heart failure than in the control group consisting of healthy control. However, there was no significant difference in abnormal capillaroscopic features between patients with reduced ejection fraction heart failure and the control group [16].
The importance of cardiac arrhythmias or blocks has been emphasized in previous studies. It has been shown that RBBB and significant arrhythmias are independent predictive factors of mortality in SSc [17, 18].
Arrhythmias are considered a contributing factor in 6% of deaths associated with SSc [19]. In our study, we found that 2 parameters of NVC reduced density and disorganization, which correlated with cardiac outcome (cardiac block or arrhythmias). However, the other 4 main parameters did not show any significant differences. We can hypothesize that the cardiac block or arrhythmias may be the result of ischemia in the conduction system. This hypothesis warrants further investigation in a cohort study.
The test Se of 94% implied that low capillary density is a strong screening tool, and high NPV suggested that in patients with normal capillary density, the likelihood of not developing a cardiac outcome was 94%. Disorganized capillaries also showed high Se (94%), PPV (80%), and NPV (85%). However, when considering 2 abnormal parameters together, both the positive likelihood ratio (LR+) and negative likelihood ratio (LR–) were low.
Study limitations
Our study had a cross-sectional design. Low capillary density and disorganized capillaroscopic features were associated with SSc-pHI, however, we cannot infer causality.
An advanced electrocardiographic evaluation, including 24-hour Holter monitoring or exercise testing, was not performed in patients with a normal resting ECG. Peak tricuspid regurgitation velocity > 3.4 m/s on echocardiography was considered a surrogate marker of PH for the diagnosis of PAH. Additionally, cardiac magnetic resonance imaging was not performed due to high cost.
Conclusions
The present study showed the prevalence of reduced capillary density and more severe capillaroscopic disorganization in patients with arrhythmias and conduction blocks. However, other semi-quantitative and quantitative parameters showed no difference. Additionally, the cardiac arrhythmias and block showed no association with the qualitative NVC patterns (normal, early, active, late). These findings suggest that physicians should pay close attention to the risk of cardiac dysrhythmias and conduction blocks in patients with SSc who exhibit decreased capillary density and disorganized capillaries.