
Introduction
The aging population is growing worldwide [1], and older adults, of whom there are more and more, require care and attention. There were 1 billion people aged over 60 years in 2019, and this number is predicted to increase to up to 2.1 billion by 2050 [2]. According to a 2015 World Health Organization report, the number of seniors over the age of 65 will be as high as 1.6 billion in 2050, representing 16.7% of the world’s population [3]. These demographic changes translate into economic and social costs [1], including increased demand for health care and treatment resources [4]. Aging is a progressive, continuous, and irreversible process. Deteriorating physical and cognitive functions contribute to an increased risk of falls in older adults [5]. Falls are a common cause of injuries and hospital admissions [3], and reduce the quality of life of this group [6]. Each year, 1 in 3 people aged ≥ 65 years and 1 in 2 people aged ≥ 80 years experience a fall [7]. Along with age, sex is also a major risk factor for falls. Being female, especially in early old age, also increases the likelihood of falls, although the sex difference becomes less pronounced in later life. If the frequency of incidents does not decrease and the aging of the population is taken into account, the number of falls among people aged ≥ 65 is expected to increase by 47% by 2050 [8]. Experiencing a first fall significantly increases the risk of subsequent falls. This can lead to various types of injuries, including head trauma and fractures. In addition, about 73% of seniors develop post-fall syndrome after an incident. Fear of another fall causes these individuals to limit their overall physical and social activity [9]. Gait and balance disturbances are modifiable and are the most common risk factors [10]. Since coordination and balance, both static and dynamic, have a huge impact on the frequency of falls in seniors, special attention should be paid to improving these components in this group [11, 12].
It is necessary to counteract health problems by focusing on preventive measures [11]. Today, seniors have access to a variety of specially designed physical activities, such as Pilates [13], Tai Chi [14], dance [15], and Zumba Gold (ZG), through which they can gain health benefits [16]. Zumba is derived from Spanish and means “have fun and move,” and was created in the 1990s. Its origins can be traced back to Colombia, where the fitness instructor Alberto Perez forgot to bring conventional aerobics music to his class and replaced it with what he had on hand, i.e., Latin music. Hence, salsa, bachata, samba, merengue, cha-cha, rumba, reggaeton, cumbia, etc., are the rhythms in ZG. Since ZG is a slower version of Zumba, based on simple and basic steps of almost every dance style, the classes can be attended by less fit and weaker individuals, or by those who are just beginning their adventure with Zumba. Zumba Gold improves aerobic capacity and balance, causes weight loss, and improves quality of life [17]. Musical activity also has a positive effect on the psyche. Calm music has a relaxing effect, reduces muscle tension, improves mood, relieves mental and physical tension, and even calms. Energetic music enhances motivation and effort, focusing on action [18]. Faster melodies, for example, speed up heartbeat and breathing, and stimulate and encourage dancing (as a form of auditory-motor exercise). Dance classes integrate people (they can laugh together, imitate each other’s movements, and exchange comments during and/or after class), reduce pain and stress, and bring joy [19–21]. Dancing activates many brain centers simultaneously [22], including those responsible for spatial movement, limb coordination, vertical balance, posture, and emotion. It therefore seems that dancing combines many of the qualities needed to slow down the aging process and may have an impact on reducing the number of falls.
The aim of this study was to investigate the effect of ZG training on static and dynamic balance, compare this training with conventional group exercises, and determine whether ZG may reduce the risk of falls in older adults. The basic assumption, the hypothesis tested, was that Zumba dancing and conventional training are comparably effective. The specific goal was to identify the differences between the two approaches.
Material and methods
Participants
The study involved 38 subjects (33 women and 5 men) aged 61 to 83, who belonged to Warsaw senior citizen clubs and had no contraindications to physical activity. The inclusion criteria for the study were age over 60 years and the ability to move independently. The exclusion criteria included moderate to severe dementia, advanced hearing loss, visual impairment, or health conditions caused by serious illness or major life events. The Physical Activity Scale for the Elderly (PASE) was used in the study to assess baseline physical activity in both groups. The duration and frequency of physical activity undertaken in the past 7 days were assessed in three domains: work, home, and recreational activities. The author’s questionnaire was also used to collect data on age, sex, body height, body mass, body mass index (BMI), current health problems, and pain based on a Numeric Rating Scale (NRS). Nineteen individuals (17 women and 2 men) participated in the ZG training, and 19 (16 women and 3 men) in the conventional balance exercise (BE) group. Assignment to groups was random, and the researcher drew a group number for each participant. The study was conducted as a single-blind intervention because it was not possible to blind the participants, but the scores of performance tests were blinded. Before the training, 6 and 5 participants from the BE and ZG groups had experienced falls in the last year: 1, 1, 1, 2, 3, 3 falls, and 1, 1, 1, 1, 2 falls, respectively. None of the study participants experienced a fall during the intervention. All subjects completed full sessions without any harm or side effects. There was no group without any training, so that all older adults participating in the study had the opportunity to improve their health.
Training sessions
Both groups participated in 10 classes, each lasting 45 minutes, three times a week. The classes were held in subgroups of four to five people, both in the BE and ZG groups. The training was conducted by the same physiotherapist who had the necessary qualifications, including a ZG instructor certificate. In both groups, the warm-up lasted 10 minutes and the stretching lasted 5 minutes. In the ZG group, the warm-up included dance movements of each body segment, steps, and coordination of the upper and lower limbs, or a combination thereof. The warm-up in the BE group was typical and included active free movements of individual joints. The main part of both training sessions lasted 30 minutes. In the ZG group, difficulty was graded by the choreography’s complexity, the rhythm’s speed, and the addition of contralateral limb movements. The session began with simple and slower choreography with less complex coordination of the upper and lower limbs, and then gradually progressed to more difficult ones. In the BE group, the increase in difficulty consisted of narrowing the body’s support plane from feet hip-width apart to a foot-over-foot position, as well as using an unstable surface and distractors such as sound, closing the eyes, and performing destabilizing tasks simultaneously. Small and large exercise balls, rehabilitation discs, and Thera-Band tapes were used for BE.
Clinical tests of static and dynamic balance
Coordination and balance, both static and dynamic, have a significant impact on the frequency of falls in older adults. Therefore, static and dynamic balance, risk of falls and functional fitness were measured under the same conditions and in the same order, the day before and after completing the entire training cycle. Static balance was assessed using clinical tests (i.e., primary outcome set) [12, 23–27], such as the Tandem Stance Test (TST) [25], and the One Leg Stance Test (OLST) Right (OLSTR) and Left (OLSTL) [12]. Dynamic balance was measured using the following clinical tests: Tandem Walk Test (TWT) [24], Tandem Pivot Test (TPT) [25], Four Square Step Test (FSST), and Functional Reach Test (FRT) [26]. The Timed Up and Go (TUG) test was used to evaluate fall risk and functional mobility [27]. In addition, posturographic measurements of static balance were taken [23]. The tests were performed twice by the same experimenter, and the average was calculated.
Table I summarizes the study’s measured and calculated parameters.
Table I
Sets of measured and calculated parameters in the study
[i] BMI – body mass index, EA – ellipse area, EC – eyes closed, EO – eyes open, FRT – Functional Reach Test, FSST – Four Square Step Test, NRS – Numeric Rating Scale, OLSTL – One Leg Stance Test Left, OLSTR – One Leg Stance Test Right, TL – total length, TPT – Tandem Pivot Test, TST – Tandem Stance Test, TWT – Tandem Walk Test, TUG – Timed Up and Go, V – velocity.
Balance tests
Static balance tests: Tandem Stance Test, One Leg Stance Test Right and Left
Static balance was assessed using three tests. The Tandem Stance Test [25], which specifies a minimum time of 10 seconds to maintain a foot-for-foot position, involves assuming a foot-for-foot (tandem) position in which the toes of the pivoting foot touch the heel of the striking foot. The performance of the task was scored on a 0–5-point scale, where 0 points meant that the subject needed assistance to hold the position and not fall over, and 5 points meant that the participant could hold the position safely and independently for 10 seconds. The OLSTR and OLSTL [12], with a cut-off point of 30 seconds, consisted of standing straight and raising one leg bent at the hip and knee to 90 degrees; the test was performed without shoes.
Dynamic balance tests: Tandem Walk Test, Tandem Pivot Test, Four Square Step Test, and Functional Reach Test
Dynamic balance was measured using four clinical tests. The Tandem Walk Test [24] consisted of walking 10 steps forward along a designated line, foot by foot (feet touching with each step). The subject was assessed on a scale of 0–5 points, where 0 meant an inability to take 1 step along the line, and 5 points corresponded to taking a minimum of 7 steps without interruption, with correct foot positioning, and performing the task in a coordinated manner. In the TPT [25], the participant assumed a foot-by-foot (tandem) position, freely choosing the front foot and performing a 180-degree pivot; after completing the task, the feet should be in the starting position. The subject was assessed on a scale of 0 to 5 points, where 0 points meant that the person was unable to assume the tandem position and perform the task independently, and 5 points meant that the person independently assumed the tandem position and performed the task in a fully coordinated manner. In the FSST [26], two intersecting lines were taped to the floor to form a square; the subject in the starting position was asked to stand in the left rear corner of the square, move to the front left corner of the square after the command “start,” then move sideways to the front right corner of the square, then back to the rear right corner of the square and move sideways to the rear left corner, and then return in reverse order to the starting point. The test was performed for a time, and the stopwatch measurement was recorded in seconds. The person was assessed while facing the examiner throughout the test. The starting position in the FRT [26] consisted of standing with legs apart on a line taped to the floor perpendicular to the wall, with the upper limb raised forward at a 90-degree angle, straightened at the elbow joint, with the hand clenched into a fist (the position of the fist was marked on the wall). The test consisted of swinging the torso forward as far as possible without losing balance, leaning against the wall, or taking a step forward, without straightening the fingers. At the moment of maximum lean, the final position was marked on the wall, and the distance covered was measured in centimeters.
Posturographic tests
Static posturography can be used as an objective tool to complement clinical balance tests to assess and control balance [23]. So, additionally, a posturographic exam was performed with a 30-second Romberg test with eyes open (EO) and eyes closed (EC), using a FreeMED Maxi tensometric mat (Coordination, Inc., Poland), as shown in Figure 1. The FreeMED Maxi consists of a plate equipped with sensors that measure the distribution of pressure force and changes in the center of pressure (COP) projection onto the XY support surface. Body sways can be recorded as a trajectory (i.e., a posturogram) representing the displacement of the COP value on the XY plane during the posturographic test [23]. The following basic parameters of the posturographic trajectory were calculated: total COP path length (TL), mean COP velocity (V), and COP ellipse area (predictive ellipse area with 95% COP values) (EA) (i.e., a set of secondary outcomes). The Romberg test is performed as follows: (a) participants stand with feet together, eyes open (EO), and arms spread out to the sides, and then (b) participants close their eyes (CE) while the examiner observes the subject for 30 seconds. An important feature of the test is that the person becomes more unstable with eyes closed.

The Timed Up and Go test
Balance exercise test for fall risk and functional mobility
The TUG test consists of the following actions, measured by time: standing up from a chair, walking 3 m to a designated line, performing a half-turn, returning the same way, and assuming a seated position with back support, all completed with a stopwatch measuring time in seconds [27]. A cutoff point of 10 seconds indicates an increased risk of falling. It is recommended to supplement the TUG test with other tests [28]. This approach was used in this study.
Statistical analysis
The statistical package STATISTICA (version 10 StatSoft Poland) and G*Power software (version 3.1.9.7 Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) were used for statistical analysis. The normality of the distribution of the analyzed variables was assessed using the Shapiro-Wilk test. The results are presented as arithmetic means with standard deviations (SD), 95% confidence intervals (95% CI), and standardized effect sizes (Cohen’s d). The significance of the observed differences was checked using the Friedman or Kruskal-Wallis test, as appropriate. When overall significance was detected, post-hoc analyses were performed using the Wilcoxon signed-rank test to compare pre- and post-intervention outcomes within each group, and the Mann-Whitney U test to compare scores between the BE and ZG groups. The χ2 test was used to assess the distribution of sex and age categories between the study groups. The size of the groups allowed for the detection of significant differences in key primary outcomes with a test power (1-β) of 0.7–0.9. A p-value < 0.05 was considered statistically significant.
Bioethical standards
The study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics Committee of the National Institute of Geriatrics, Rheumatology and Rehabilitation in Warsaw (approval No. KBT-5/5/23 06.12.2023). The rules of the study were explained to the participants, and they were informed that they could withdraw at any time without giving any reason and without any consequences. Written consent to participate in the study was obtained from each subject.
Results
The characteristics of the BE group and the ZG group are shown in Table II.
Table II
Characteristics of the research groups before the training
The mean age of the subjects was 73 ±6 years (95% CI: 71–75), mean body mass was 70 ±14 kg (95% CI: 65–74), and mean body height was 1.6 ±0.1 m (95% CI: 1.6–1.7). The PASE score was 132 ±61 (95% CI: 103–161) in the ZG group and 109 ±41 (95% CI: 90–129) in the BE group, so physical activity was slightly higher in the ZG group (p = 0.181). Pain was reported by 31 participants (82%). Back pain was the most common, followed by shoulder/arm pain (4 subjects), knee pain (3), thumb pain (1), and multi-joint pain (1). Seven participants experienced no pain (18%). Before the training, the mean pain level was 4.7 ±1.9, which significantly decreased after the training to 2.7 ±2.1 (95% CI: 4.0–5.4 vs. 1.8–3.5; p < 0.0001). However, nine patients reported no change in pain after the training. Significant reductions in pain were observed in both groups, from 4.5 ±1.8 to 2.9 ±2.3 in BE (95% CI: 3.5–5.6 vs. 1.5–4.3; p = 0.002) and from 4.9 ±2.0 to 2.4 ±2.0 in ZG (95% CI: 3.8–5.9 vs. 1.4–3.5; p = 0.0004). However, the differences between the groups were not statistically significant.
In both groups, a significant improvement in clinical (primary) outcomes was observed, as shown in Table III.
Table III
Clinical test results as mean values with SD before and after the training with standardized effect sizes (Cohen’s d) in the balance exercise (BE) and Zumba Gold (ZG) groups
| Clinical tests | BE group (n = 19) | ZG group (n = 19) | ||
|---|---|---|---|---|
| Before vs. after | Cohen’s d [1-β] | Before vs. after | Cohen’s d [1-β] | |
| Fall risk | ||||
| TUG test [s] | 7.8 ±2.4 vs. 7.2 ±1.6* | 0.59 [0.78] | 6.7 ±1.3 vs. 6.0 ±1.1*** | 0.71 [0.89] |
| Static balance | ||||
| TST (points) | 3.9 ±1.5 vs. 4.5 ±1.2* | 0.58 [0.77] | 4.6 ±0.8 vs. 5.0 ±0.0* | 0.51 [0.67] |
| OLSTR [s] | 11.7 ±10.4 vs. 17.1 ±11.3* | 0.46 [0.59] | 22.4 ±10.1 vs. 27.7 ±4.6* | 0.55 [0.73] |
| OLSTL [s] | 11.7 ±11.7 vs. 14.2 ±10.6 | 0.38 [0.46] | 23.7 ±8.2 vs. 26.8 ±6.1 | 0.43 [0.54] |
| Dynamic balance | ||||
| TWT (points) | 3.2 ±1.4 vs. 4.0 ±0.5* | 0.54 [0.71] | 4.0 ±1.1 vs. 4.7 ±0.5* | 0.54 [0.71] |
| TPT (points) | 2.8 ±1.0 vs. 3.7 ±1.2** | 0.70 [0.89] | 3.7 ±0.9 vs. 4.5 ±0.6** | 0.62 [0.81] |
| FSST [s] | 10.0 ±3.1 vs. 7.9 ±1.8***, # | 0.86 [0.97] | 7.8 ±1.2 vs. 6.9 ±1.3*** | 0.74 [0.92] |
| FRT [cm] | 30.1 ±7.2 vs. 35.0 ±3.9** | 0.66 [0.85] | 34.6 ±4.9 vs. 39.9 ±5.0*** | 0.82 [0.95] |
[i] Significant levels: *p < 0.05, **p < 0.01, ***p < 0.001 for pre- and post-training comparisons, and #p < 0.001 for between-group comparisons after the training; arithmetic mean values with standard deviations (SD), standardized effect sizes reported as Cohen’s d (i.e., 0.1 small, > 0.3 medium, > 0.5 strong, or > 0.7 very strong effects), and test power [1-β] for the Wilcoxon rank-sum test are given.
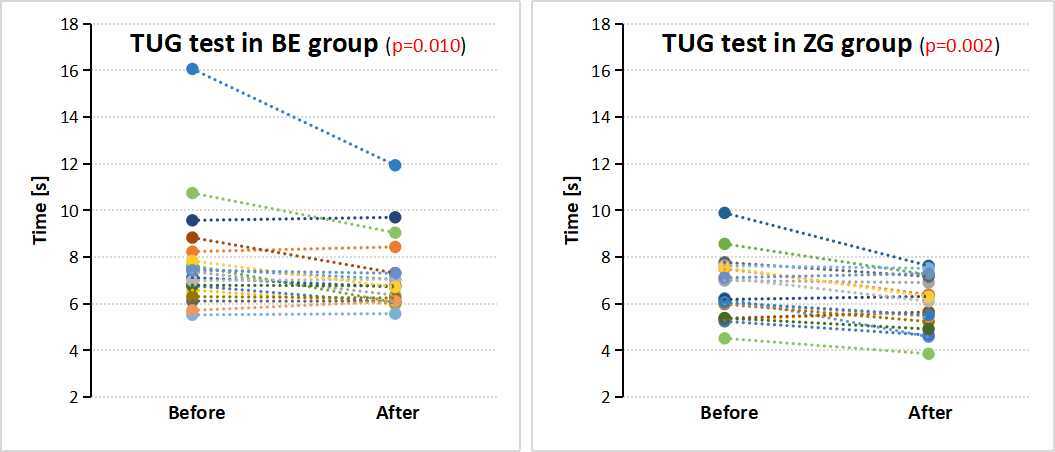
The TUG test performed before and after training in both groups showed statistically significant improvement for ZG (95% CI: 6.0–7.3 vs. 5.5–6.5; p = 0.002) and BE (95% CI: 6.7–9.0 vs. 6.4–7.9; p = 0.010). Figure 2 also shows the TUG test results for each participant in both groups. Tandem tests also presented significant improvement: (a) TST in ZG (95% CI: 4.2–4.9 vs. 5.0; p = 0.028) and BE (95% CI: 3.2–4.7 vs. 3.9–5.1; p = 0.012); (b) TWT in ZG (95% CI: 3.5–4.5 vs. 4.5–4.9; p = 0.018) and BE (95% CI: 2.5–3.9 vs. 3.3–4.3; p = 0.018); (c) TPT in ZG (95% CI: 3.3–4.2 vs. 4.2–4.8; p = 0.007) and BE (95% CI: 2.3–3.3 vs. 3.1–4.3; p = 0.002). Subsequent tests with significant improvement included the FSST in ZG (95% CI: 7.2–8.3 vs. 6.3–7.5; p = 0.001) and BE (95% CI: 8.5–11.5 vs. 7.1–8.8; p = 0.0002); FRT in ZG (95% CI: 32.3–37.0 vs. 37.5–42.3; p = 0.0003) and BE (95% CI: 26.6–33.6 vs. 33.1–36.9; p = 0.004); and the OLSTR in ZG (95% CI: 17.5–27.2 vs. 25.4–29.9; p = 0.017) and in BE (95% CI: 6.7–16.7 vs. 11.6–22.5; p = 0.044). No significant improvement was achieved in OLSTL alone in either group. There were no statistically significant differences in clinical tests between groups, except for FSST, where a statistically significant improvement was observed in the BE vs. ZG group (p = 0.012). In another analysis of the effect size parameter, strong effect sizes were observed for the TUG test, TPT, and FRT tests, while the strongest effect size occurred for the FSST in the BE group. The values for the TWT and OLST tests were lower, and were the lowest for the OLSTL test in both groups. These results indicate favorable changes in dynamic balance tests (except TWT) compared to static balance tests. Improving static and dynamic balance has been shown to reduce the risk of falling, as observed in the study.
Fig. 2
Timed Up and Go test results for each participant before and after training in the balance exercise (BE) and Zumba Gold (ZG) groups.
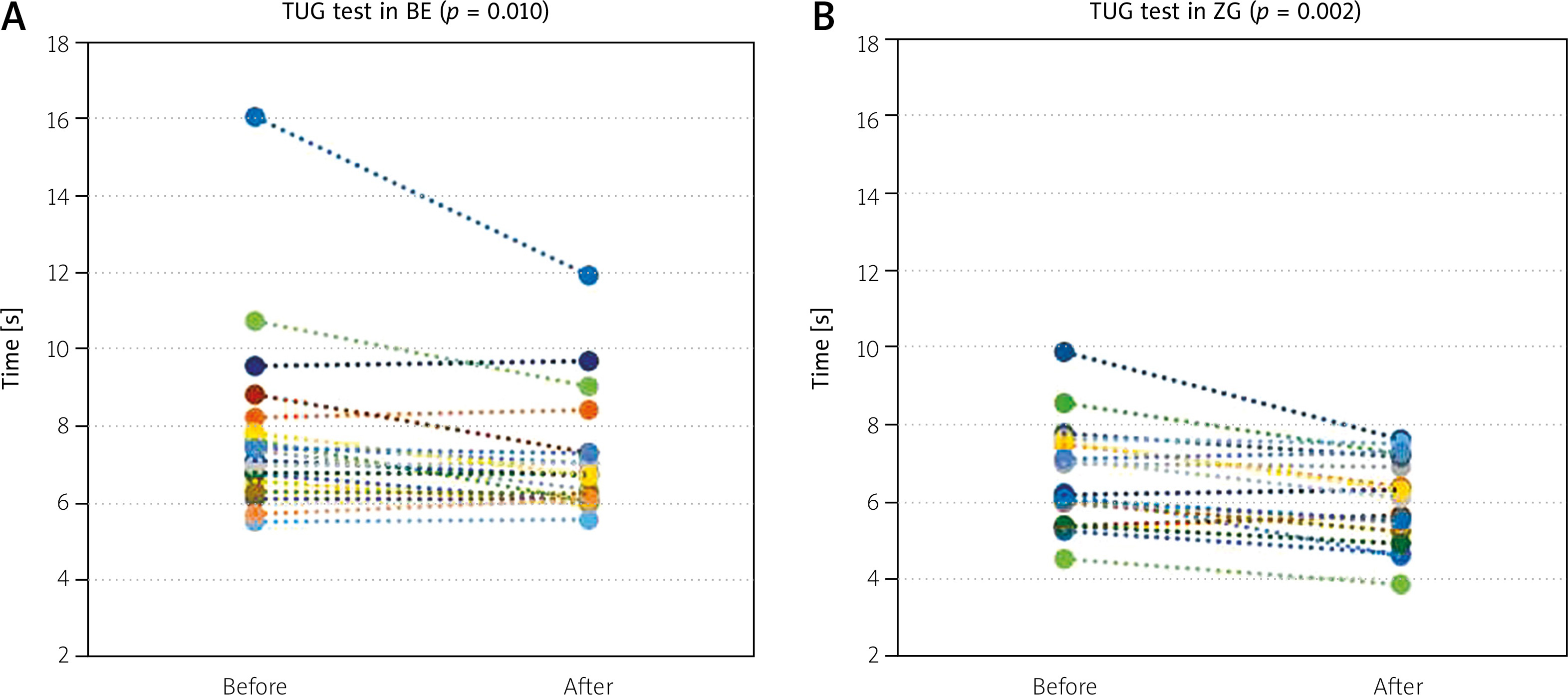
Table IV presents posturographic scores from the Romberg test with eyes open and closed in both groups before and after training (the set of clinical secondary outcomes).
Table IV
Posturographic test results as mean values with SD before and after the training in the balance exercise (BE) and Zumba Gold (ZG) groups
In posturographic tests for TL and V parameters in the ZG group, improvement was observed after training compared to the BE group, but it was not statistically significant.
Discussion
Zumba Gold offers health benefits, including improved functional fitness and mood, as well as cognitive function, attention, and memory [15]. Exercises focusing on balance, lower limb strength, and coordination are among the most effective forms of physical activity for preventing falls in older adults [5]. They reduce the risk of falls by 23–28%. The most optimal outcomes were achieved with multi-component training performed 3 times a week for 1 hour for 16 weeks, as it increased balance by 42% [11]. In our study, a 10.7% and 8.2% TUG test improvement in the ZG and BE groups, respectively, was achieved after just 10 sessions. Subsequently, for static balance, the TST showed improvement in the ZG and BE groups. Zhao et al. [29] found that Tai Chi produced better results than BE. In their study, TUG test scores decreased by 1 s after the Tai Chi intervention, while the improvement was 0.14 s after balance training. In the study by Kasim et al. [14], the applied training reduced TUG test performance time by 0.8 s; the result was statistically significant (p = 0.004) in the Zumba group but not in the Tai Chi group. In our study, TUG scores decreased by 0.7 s in both groups (p = 0.002 for ZG, p = 0.010 for BE). The effects of therapy using different dance styles and their beneficial impact on improving balance and reducing the risk of falls have also been described. Mishra Siddharth and Shukla [30] reported that Indian folk-dance therapy led to a significant increase in single-leg stance time. Flamenco dance therapy resulted in a significant improvement in TUG test by 1.8 s (p = 0.02) and OLST by 7.6 s (p = 0.001) [31]. Argentine tango therapy also had a positive effect on reducing the risk of falls in TUG test, with a difference of 1.3 s (p = 0.003) [32]. Similarly, Rocha et al. [33] reported an improvement in TUG test of 1.69 (p = 0.037) after dance therapy.
Improvements in balance were also noted when combining elements of different dance styles. Chulvi-Medrano et al. [34], Ogaya et al. [35], and Dunsky et al. [36] compared non-standard forms of physical activity in the prevention of falls in seniors, obtaining results similar to dance therapy. Various equipment was used, e.g., the T-Bow board, the Wobbel board, step aerobics (SA), and a stability ball. It was found that exercises with the T-Bow board resulted in a 35.2% improvement in static balance in the OLST test. After 8 weeks of training, a 12.7% reduction in the risk of falls in TUG was also demonstrated, and the results were statistically significant (p = 0.005) [34]. Other authors reported a 37.8% improvement in OLST after 9 weeks of training with the Wobbel board, while TUG time increased by 1 s and FRT score worsened by 3.4 cm [35]. In our study, the FRT parameter improved significantly by 5.3 cm (p < 0.001) after ZG therapy. The study by Dunsky et al. [36] found that SA is a better therapy than stability ball exercises in reducing the risk of falls, with the SA group showing a significant improvement in the TUG test of 1.4 s (p = 0.01). The improvement was not statistically significant in OLSTR and OLSTL. Given the similarity of the interventions in Dunsky’s study and ours (ZG vs. SA and group exercise vs. stability ball exercise), an attempt was made to compare them. Analyzing the results of both studies in the ZG and SA groups, a significant reduction in the risk of falls was found. Comparing the outcomes in the BE group with the stability ball exercise group, we found that our exercises were more effective, as evidenced by statistically significant results in TUG test with an improvement of 0.7 s (p < 0.05), an improvement of 4.9 cm (p = 0.001) in FRT, and an improvement of 2.5 s (p = 0.03) in OLSTR, as well as a slight improvement after ball exercises in TUG test by 0.6 s and OLSTR by 1.3 s, and a worsening in FRT by 0.8 cm, which may suggest that greater variety of equipment used, the use of an unstable surface, and a change in the support surface have greater benefits for body balance. Virtual reality technology is increasingly being used in fall prevention. Comparing the posturography results after virtual reality therapy (VRT) with those in the ZG group, a reduction in the total length of swings of 35 mm (14.1%) was observed, compared to only 13 mm (5.1%) after VRT [37]. The risk of falls in the ZG group decreased by 10.7% in the TUG test (p < 0.0001) and by 9.9% (p = 0.01) in VRT.
Reports of physical activity among seniors most often indicate low-level activity. Delextrat et al. [38] measured seniors’ physical activity using the PASE scale before the ZG intervention, similar to our study. The mean age of the subjects was 64 years, and the median PASE score was 78.9. In this study, the mean age of the ZG participants was 70.6 years, and the median PASE score was 130.8. This shows that people of different ages and with varying levels of daily activity can participate in ZG classes and experience health benefits after only 6 classes. Pain is one of the determinants of an increased risk of falls. Many seniors struggle with various types of pain in their muscles, joints, and other body structures. Lee found that music reduces pain by 1.1 on the NRS scale [20]. In this study, a significant reduction in pain was observed in both groups, but it was 0.9 times higher in the ZG group. According to a review of therapies using various exercises conducted by Thomas and Lane [12], it is not the type of training that is important, but the exercise itself. Any physical activity is recommended to prevent falls. However, some forms of activity may be preferred by older people due to their specific nature, which is attractive to them. It is worth recalling Erikson’s view on older people who, for example, thanks to their interest in innovation, caring for their health, and curiosity about the world, find it easier to resolve the integration-desperation crisis [39]. Openness to change, a belief in improving one’s psycho-physical condition, and a willingness to interact with others, including doctors and physiotherapists, as well as through technical innovations and new working methods, are manifestations of integration. Signs of despair, on the other hand, include giving up on trying to change one’s situation, believing that there is too little time left to take care of oneself and one’s health, reluctance to try new working methods, and complaining about the need for change. It should be noted that the eighth and ninth stages of Erikson’s psychosocial development, occurring in late adulthood (from 55 to 65 years of age until death), summarize life, allow one to understand its meaning, and evaluate one’s life path [40]. Therefore, it is worth supporting everything that encourages participation and does not cause older people to give up activities.
It should be noted that older adults enjoy music classes, listening to favorite melodies, or using predictable and familiar rhythms. Dance training is most effective when the music is acceptable, not too loud or too quiet, and rhythmically engaging, promoting movements that are well coordinated with the music. Dancing also requires focus and concentration on the movements and memorizing them so that they are performed in harmony with the melody. Participants also have the opportunity to forget their problems, relax, and get away from everyday life for a while. Zumba exercises, like other exercise classes with dynamic music, can be considered an active form of leisure. Such activities can also be part of music therapy, especially in the case of neurodevelopmental and neurodegenerative disorders [41]. In this context, it is worth emphasizing that the study highlights the need to find new and interesting ways to activate seniors. All subjects were engaged in the training, and the ZG group spontaneously expressed enjoyment of this form of exercise, combined with dancing and a change of scenery, and a more socialized training than the traditional one. The novelty effect and an attractive “break” from routine may play a role here. Observations of the emotions experienced and self-observation of these emotions during exercise can be further analyzed. However, this increases the time burden on physical therapists as well as participants, who have additional responsibilities (recording). Therefore, this requirement no longer appears in many studies. This does not mean, however, that the emotional-motivational elements are unimportant. They certainly influenced the participants enough for them to persevere in the study.
Study limitations
This study was a single-blind exercise intervention because it was not possible to conceal the group assignment from the participants. Furthermore, due to the limited sample size, caution should be exercised when generalizing these results to a larger population. Limitations also include the varied age distribution of the seniors studied; the predominance of individuals at low risk of falling, e.g., TUG scores below ten seconds, although 11 of the 38 participants (29%) had experienced falls before the intervention; and the small percentage of men compared to women. Therefore, the effects of sex and advanced age were not evaluated in this study.
Overall, from a scientific point of view, it should be emphasized that ZG requires further research among older adults, including studies on larger groups and in the context of the long-lasting effects of the intervention.
Conclusions
Firstly, from a methodological point of view, a set of static and dynamic balance tests and the TUG test measuring functional performance and fall risk were used to evaluate the effectiveness of training approaches based on conventional balance exercise and ZG dance. The study showed that both training methods significantly improved both static and dynamic balance, significantly reducing TUG scores in older adults. Furthermore, ZG training, like other physical activities with dynamic music, can be considered an active form of leisure activity.
Secondly, in terms of practical recommendations, the research demonstrated that dance training with ZG has a positive effect on static and dynamic balance and may be included in a recommended physical activity program to prevent falls in seniors. Just 10 classes are enough to notice physical benefits that may reduce the risk of falls and improve functional mobility. Zumba Gold and conventional BE showed similar effectiveness.
Thirdly, from a scientific perspective, future research on this topic may yield equally promising results thanks to the use of innovative technologies such as extended reality (virtual, augmented, or mixed reality), which can expand the range of activities offered to include equally interesting and engaging remote home workouts. Such novel, combined approaches undoubtedly broaden the scope of physical activity incorporating cognitive elements (through digital/mobile technologies) and further enable the popularization of new forms of health-promoting activity among older adults. These are forward-looking directions aimed at consciously improving the quality of life of seniors by maximizing their engagement.