
Introduction
One treatment method used in spinal pain syndromes is dry needling (DN), which involves the insertion of a thin, solid needle into the tissue without anesthesia or injections [1]. Needle therapy has been found to be a safe technique with few incidents of undesirable effects [2, 3]. The use of the DN technique causes immediate activation of the sympathetic nervous system, which is associated with stress-induced analgesia mechanisms. It has been shown to reduce mechanical hyperalgesia at the application sites as well as at distant sites [4]. The therapeutic effect of DN is associated with a change in the mechanical sensitivity of muscle tissue, improvement in the range of motion, reduction of muscle tension, and pain relief in patients with musculoskeletal dysfunctions [5, 6]. The therapeutic effect of DN is attributed to pain modulation mechanisms, such as local release of endogenous opioids and action consistent with the gate control theory. These processes play an important role in the reduction of nociceptive stimuli, leading to the inhibition of neuroplastic changes accompanying central sensitization at the level of dorsal horn cells of the spinal cord [7, 8].
Many scientists undertake research on the use of the DN method in low back pain (LBP), but the obtained results are ambiguous and do not fully meet the assumptions of evidence-based physiotherapy [9, 10].
In their meta-analysis, Gattie et al. [5] reported very low and moderate evidence for a significant effect of DN on functional capacity in the short term. In long-term observations, DN was not superior to other treatment methods. The authors also highlighted the lack of guidance on the techniques and dosage of DN, emphasizing the need to verify the effectiveness of DN and investigate its long-term effectiveness. The scoping review of the DN method in spine disorders by Funk et al. [11] showed that DN was mainly used for the therapy of myofascial structures. Most of the studies included in the analysis concerned a single treatment. According to the American scientists, it is necessary to conduct research to determine the parameters of the treatments (including the duration and frequency of DN) and which assessment tools are best suited to assess therapeutic progress.
From the mentioned reports, it can be concluded that the effectiveness of DN is still controversial. Most studies included a small number of participants, assessed short-term outcomes, and often investigated only a single application of DN.
In the classic approach to DN, the procedure focuses on locally treating trigger points within a single muscle, typically using a deep puncture technique. The goal is to induce a local contractile response (LTR) to deactivate the trigger point, thereby reducing pain, improving blood flow, and relaxing the tense muscle structure [12].
Another method of therapy using DN is the DN technique according to the Five Regulatory Systems Concept (FRSc), which was used for DN procedures in our study. The FRSc concept assumes that the effectiveness of therapy is based on the simultaneous consideration and regulation of 5 main systems: fascial, nervous, musculoskeletal, circulatory-respiratory, and psychosomatic. The FRSc treats the body as a complex network of functional and structural connections. The FRSc-based therapy involves the targeted application of needles to sites of regulatory dysfunction, which may be local or distant (e.g., within myofascial chains), and their selection is based on prior functional clinical analysis. This approach enables global modulation of tissue tension, normalization of muscle activation patterns, and support for the body’s autoregulatory processes [13].
The aim of the study was to evaluate the effect of DN therapy according to the FRSc on hip joint range of motion as a component of functional performance in patients with chronic LBP.
Material and methods
Study design
The research was conducted at the Clinical Research Laboratory of the Institute of Health Sciences, University of Opole. The study was registered in the International Standard Randomized Controlled Trial Number (ISRCTN) registry database (No. ISRCTN16627714).
Randomization and blinding
Participants were screened and enrolled in the study by a team consisting of an internist, radiologist, neurologist, neurosurgeon, orthopedist, and physiotherapist. Participants were randomly assigned to one of 2 groups – the study or the control group – by simple randomization in a 1 : 1 ratio using computer sequence randomization on the random.org website. Therapists performing the therapy and measurements had no contact with the team responsible for enrollment or the persons who analyzed the obtained results. The outcome assessors and data analysts did not know the patient’s identity and had no contact with the study participants.
Participants
Patients with discopathy at the L5–S1 level and chronic pain (duration at least 3 months) were eligible. Included subjects were of legal age and had a valid Modic classification in the L5–S1 section. They had not previously undergone DN procedures, and no surgical intervention in the spine was performed.
The exclusion criteria were: no pain or decreased mobility in the lumbar-sacral spine, other spine disorders (spondylolisthesis, fractures, tumors, infection, rheumatic diseases, cauda equina syndrome), advanced scoliosis, pregnancy, implanted pacemaker, blood clotting disorders, use of anticoagulant therapy, glucocorticosteroid therapy, metal implants in the area of application, sensory disorders, mental disorders, tumors, skin lesions in the area of the procedure, viral and bacterial infections, fever, use of painkillers and anti-inflammatory drugs, fear of needles, and lack of consent to the procedure.
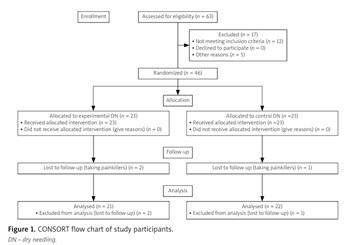
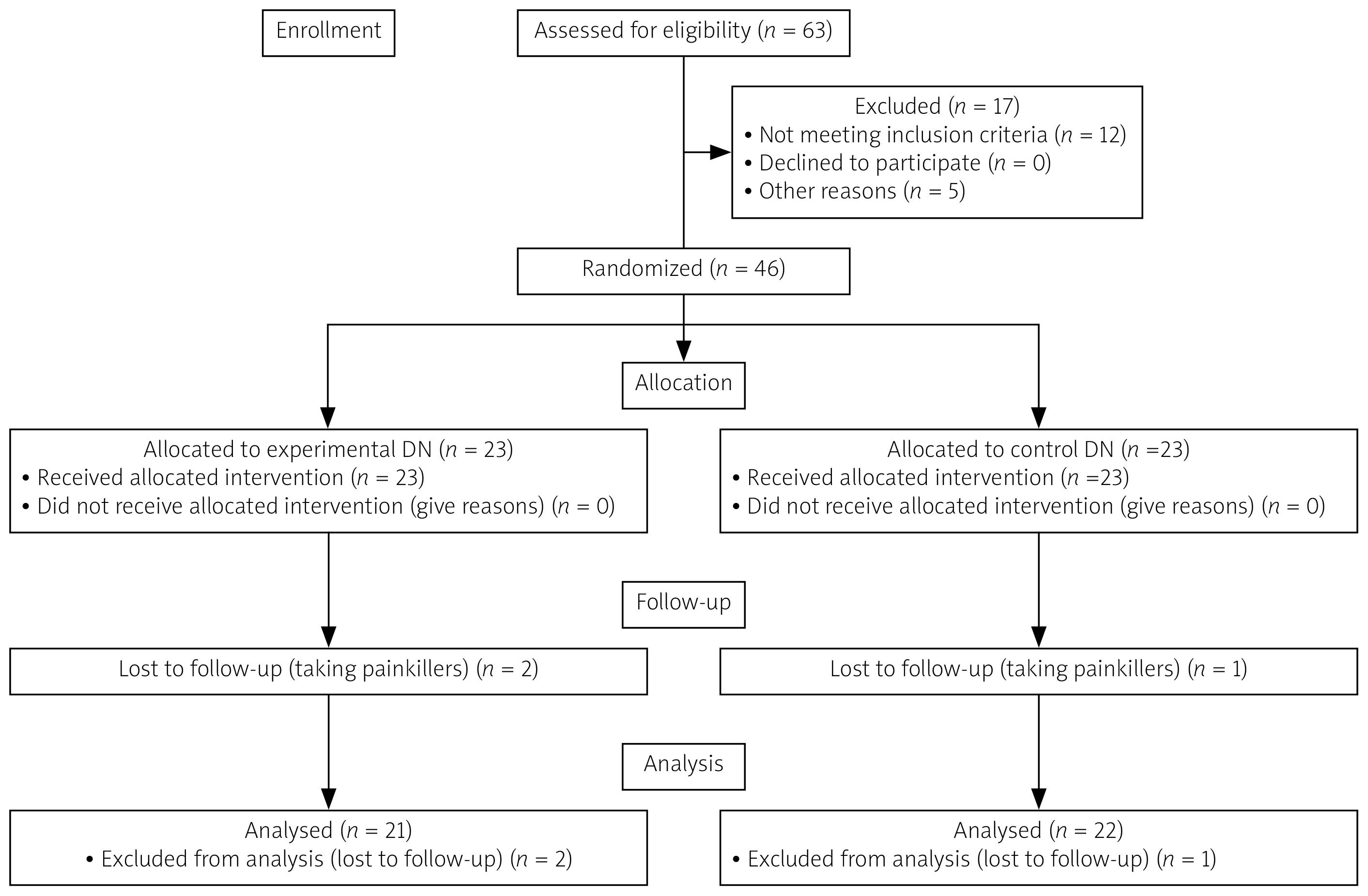
A total of 46 patients with LBP participated in the study. A homogeneous group of patients in terms of basic demographic characteristics was randomly assigned to 2 comparative groups: A (n = 23) and B (n = 23). In both groups, all patients completed the treatment. From the statistical analysis, 2 people from group A and 1 person from group B were excluded – the use of painkillers was recorded. This loss may have been associated with a risk of bias, so analyses were conducted according to the intention-to-treat principle and supplemented with a per-protocol analysis. The results of both approaches were generally consistent, suggesting that the impact of these exclusions on the final study conclusions was limited.
In accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines for registered randomized clinical trials, the flow of participants at each stage of the project is presented in Figure 1.
Interventions
In group A (DN), participants underwent DN procedures according to the FRSc using disposable, sterile needles (SOMA, China) made of Japanese surgical steel. A single procedure covered 4 anatomical areas and lasted 60 minutes. Soft tissue was punctured along the L1–L5 segment on both sides of the spine, within the palpable thickenings in the region of the groove between the spinous processes and the erector spinae muscle. Needles (75 mm) were inserted at a 30° angle until bony contact was achieved, using the “pumping” technique, with 15-minute intervals. Additionally, transverse bands of connective tissue within the erector spinae were punctured (30 mm needles) perpendicular to the skin surface, using the needle rotation technique to stop needle movement. Subsequently, the neural compartment of the superior gluteal nerve and the gluteus maximus, medius, and tensor fasciae latae muscles were activated using 100 mm needles and the “pumping” technique to obtain LTRs. The final step involved puncturing the piriformis muscle at the palpable myogelosis site, also using the “pumping” technique (100 mm needles), until at least 2 local contractions were achieved. After completing the stimulation series, the needle remained in place for approximately 15 minutes without further manipulation. The detailed application procedure was presented in our previous studies [14, 15].
In group B (control), sham treatment was administered using telescopic placebo needles that did not pierce the skin. The duration of a single treatment was the same as in group A (DN). Application locations were determined by palpation, identical to the study group. Spacer rings were placed at the designated points and then secured with thin tape. Placebo needles were inserted through the discs, retracting upon contact with the skin, allowing for gentle movements that mimicked the actual treatment without disrupting tissue continuity. In order to assess the placebo effect, this group was single-blinded.
In both groups, a total of 8 treatments were performed, which were carried out twice a week for a period 4 weeks (a single treatment lasted 60 minutes). All applications were performed by an experienced physiotherapist and instructor with naturopathic qualifications. The treatments were carried out using safety and hygiene principles, using the necessary aseptic measures on the treatment area.
Both study groups participated in an exercise program tailored to individuals with chronic LBP. The program aimed to improve core stability, posture, and breathing patterns. Exercises were performed for 4 weeks, 5 times per week (Monday through Friday), in 45-minute sessions. The therapeutic protocol included myofascial release techniques, activation of the lumbosacral-iliac complex, back muscle strengthening, respiratory training (including diaphragmatic mechanics), activation of the transverse abdominis muscle, and elements of postural training. All exercises were performed within a pain-free range, under the supervision of a therapist. The intensity and number of repetitions were individually adjusted.
Data sources and measurements
The range of motion of the hip joints of both limbs was measured using an electronic goniometer (K-FORCE, France).
In both groups, all measurements were performed before and immediately after treatment, as well as at 1- and 3-month follow-ups. All measurements were performed by experienced physiotherapists. The measurements were performed in 3 trials, which allowed for the elimination of possible errors during measurements. During this time, patients were not receiving any other therapy (pharmacology, physiotherapy) that could have influenced the project results.
Sample size
The sample size was determined assuming a large effect size (Cohen’s d = 0.8) at a significance level of α = 0.05 and 80% power. Calculations indicated that at least 23 patients per group (46 total) were needed, with a 10% loss to follow-up factor to maintain study power. Calculations were performed using the Statistica 13 package (TIBCO, Inc., USA).
Statistical analysis
Statistical analysis was performed using Statistica 13 (TIBCO, Inc., USA). For measurable variables, arithmetic means, medians, standard deviations, quartiles, and the range of variability (extreme values) were calculated. Frequencies were calculated for qualitative variables (results are given in percentages). The distribution of quantitative variables was assessed using the Shapiro-Wilk test. Comparison of qualitative variables between groups was performed using the χ2 test. Intragroup comparison between results was performed using Friedman’s analysis of variance and post-hoc test (Dunn’s test). Finally, the comparison of results between the study group and placebo was assessed using the Mann-Whitney U-test. The level of α = 0.05 was used for all comparisons.
Bioethical standards
The research was approved by the Bioethics Committee of the Public Higher Professional Medical School in Opole, Poland (approval number: KB/91/FI/2018). The studies were conducted in accordance with the guidelines of the Declaration of Helsinki and good clinical practice. All participants gave written informed consent to participate in the study.
Results
Patients in both groups were homogeneous with respect to anthropometric characteristics (Table I). Results for the study and control groups were reported for 4 consecutive time points: before therapy, after therapy, and at 1-month and 3-month follow-ups.
Table I
Characteristics of participants
| Variable | Experimental DN group (n = 21) | Control DN group (n = 22) | p | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| x | Me | Min | Max | Q1 | Q3 | SD | x | Me | Min | Max | Q1 | Q3 | SD | ||
| Age [years] | 44.4 | 43.0 | 29.0 | 60.0 | 38.0 | 50.0 | 8.2 | 51.0 | 55.0 | 29.0 | 72.0 | 38.3 | 60.0 | 13.0 | 0.070* |
| Body mass [kg] | 72.0 | 72.0 | 57.0 | 88.0 | 63.0 | 83.0 | 10.8 | 70.7 | 66.0 | 51.0 | 92.0 | 62.3 | 82.8 | 12.7 | 0.770* |
| Body height [cm] | 172.5 | 171.0 | 163.0 | 186.0 | 166.0 | 178.0 | 6.8 | 168.9 | 170.0 | 152.0 | 183.0 | 159.0 | 175.8 | 9.1 | 0.300* |
| BMI [kg/m2] | 24.2 | 23.5 | 19.9 | 30.1 | 21.8 | 27.1 | 3.2 | 24.7 | 25.1 | 19.1 | 30.1 | 21.8 | 26.7 | 3.1 | 0.618* |
| Sex | F (n = 10), 47.6% M (n = 11), 52.5% | F (n = 12), 54.5% M (n = 10), 45.5% | 0.649** | ||||||||||||
Table II presents a comparison of changes in results for range of motion of the hip joint right limb in the group undergoing DN therapy and in the control group. Baseline results (ranges of motion) in the DN group were higher than in the control group, and a favorable clinical effect was observed in both groups when assessed immediately after therapy. There were statistically significant differences in both groups (main effect: p < 0.05). In the study group, a significant increase in the score of 15.3 points was observed after the completed therapy, followed by a slight decrease of 1.3 points after 1 month and by another 1.7 points after 3 months of follow-up, reaching a final improvement of 12.3 points. In the control group, the greatest increase in the score was observed immediately after the completed therapy, by 15 points, but in the long-term follow-up the results deteriorated by 14.3 points after 1 month and by another 2.5 points after 3 months of follow-up.
Table II
Range of motion (right side) scores in both groups
| Variable | Measure | Experimental DN group | Control DN group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| x | Me | Min | Max | Q1 | Q3 | SD | x | Me | Min | Max | Q1 | Q3 | SD | ||
| Range of motion score | Before | 60.5 | 60.0 | 40.0 | 80.0 | 52.5 | 67.5 | 12.7 | 41.8 | 30.0 | 30.0 | 75.0 | 30.0 | 57.5 | 15.7 |
| After | 75.8 | 75.0 | 50.0 | 90.0 | 72.5 | 85.0 | 12.1 | 56.8 | 57.5 | 40.0 | 80.0 | 47.5 | 60.0 | 11.4 | |
| 1-month FU | 74.5 | 75.0 | 50.0 | 90.0 | 70.0 | 80.0 | 12.1 | 42.5 | 37.5 | 35.0 | 65.0 | 35.0 | 50.0 | 10.3 | |
| 3-month FU | 72.8 | 75.0 | 50.0 | 90.0 | 70.0 | 80.0 | 11.8 | 40.0 | 35.0 | 30.0 | 65.0 | 30.0 | 50.0 | 12.4 | |
| p-value (main effect*) | < 0.001 | < 0.001 | |||||||||||||
| p-value (multiple comparisons**) | Before vs. after: p < 0.001 Before vs. 1 month: p < 0.001 Before vs. 3 months: p < 0.001 After vs. 1 month: p = 0.021 After vs. 3 months: p < 0.001 1 month vs. 3 months: p = 0.005 | Before vs. after: p < 0.001 Before vs. 1 month: p = 0.751 Before vs. 3 months: p = 0.427 After vs. 1 month: p < 0.001 After vs. 3 months: p < 0.001 1 month vs. 3 months: p < 0.001 | |||||||||||||
Table III presents a comparison of changes in results of range of motion of the hip joint left limb in the group undergoing DN therapy and in the control group. Baseline results (ranges of motion) in the DN group were higher than in the control group, and a favorable clinical effect was observed in both groups when assessed immediately after therapy. There were statistically significant differences in both groups (main effect: p < 0.05). In the study group, a significant increase in the score of 13 points was observed after the completed therapy, followed by a slight decrease of 1.3 points after 1 month and by another 1.7 points after 3 months of follow-up, reaching a final improvement of 10 points. In the case of the control group, the greatest increase in the score was observed immediately after the completed therapy, by 18 points, but in the long-term follow-up the results deteriorated by 20.7 points after 1 month and by another 1.8 points after 3 months of follow-up.
Table III
Range of motion (left side) scores in both groups
| Variable | Measure | Experimental DN group | Control DN group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| x | Me | Min | Max | Q1 | Q3 | SD | x | Me | Min | Max | Q1 | Q3 | SD | ||
| Range of motion score | Before | 59.8 | 60.0 | 25.0 | 85.0 | 50.0 | 72.5 | 17.2 | 43.5 | 37.5 | 25.0 | 80.0 | 30.0 | 57.5 | 16.0 |
| After | 72.8 | 80.0 | 30.0 | 90.0 | 70.0 | 80.0 | 17.0 | 61.5 | 60.0 | 45.0 | 80.0 | 52.5 | 70.0 | 11.6 | |
| 1-month FU | 71.5 | 75.0 | 30.0 | 90.0 | 70.0 | 80.0 | 16.6 | 40.8 | 37.5 | 25.0 | 60.0 | 35.0 | 45.0 | 9.4 | |
| 3-month FU | 69.8 | 75.0 | 30.0 | 90.0 | 60.0 | 77.5 | 16.9 | 39.0 | 37.5 | 25.0 | 60.0 | 30.0 | 45.0 | 10.7 | |
| p-value (main effect*) | < 0.001 | < 0.001 | |||||||||||||
| p-value (multiple comparisons**) | Before vs. after: p < 0.001 Before vs. 1 month: p < 0.001 Before vs. 3 months: p = 0.001 After vs. 1 month: p = 0.021 After vs. 3 months: p < 0.001 1 month vs. 3 months: p = 0.031 | Before vs. after: p < 0.001 Before vs. 1 month: p = 0.334 Before vs. 3 months: p = 0.095 After vs. 1 month: p < 0.001 After vs. 3 months: p < 0.001 1 month vs. 3 months: p = 0.005 | |||||||||||||
Discussion
The present single-blind randomized clinical trial was conducted to investigate the effect of DN according to the FRSc on range of motion of the hip joints as an element of functional performance in patients with LBP. The study protocol included a homogeneous population of LBP patients in terms of the analysis of the range of motion of both lower limbs. In both groups, all measurements were taken before and immediately after treatment. To verify the results, follow-up measurements were also performed 1 and 3 months after the end of therapy.
The positive effects of DN therapy on functional outcomes are indicated by the results presented by Padanilam et al. [12], who recommend this technique as a minimally invasive therapeutic method. The authors emphasize that DN provides significant short-term improvement in function and analgesic effect in the case of musculoskeletal complaints. The effectiveness of DN in the treatment of LBP was confirmed by Mahmoudzadeh et al. [16] in a randomized clinical trial. Patients were divided into a group receiving standard physiotherapy and a group in which physiotherapy was supplemented with DN. After 10 therapeutic sessions, conducted every other day, a reduction in pain and disability was noted in both groups, which was maintained after 2 months. The authors indicate that the addition of DN may enhance the effect of standard therapy. The positive effects of DN in patients with LBP were demonstrated in the study by Deshpande et al. [17]. Forty patients were enrolled in the project. Patients with LBP underwent 5 DN sessions (20 minutes each, every 3 days). The authors noted significant improvements in functional outcomes and pain reduction, persisting for up to 12 weeks after the intervention. The positive impact of DN therapy in patients with LBP has also been reported by other studies [18–20].
Researchers have demonstrated that hip range of motion plays an important role in assessing pain and mobility in patients with LBP. In a 2023 meta-analysis, researchers from Spain emphasized that the lumbar spine is connected to the pelvis and hips, so LBP may be directly or indirectly related to the limitation of the range of motion of the spine and hip movements. Therapists should consider assessing the hip joint area in patients with LBP [21]. Also, Pizol et al. [22] in their systematic review, reported that patients with LBP, regardless of symptoms, showed a significant reduction in the range of hip joint movement during specific tests and functional activities compared to healthy individuals. Miyachi et al. [23] observed relationships between LBP and lumbar spine and hip movement. Prather et al. [24] in their study compared pain and function in patients with LBP. The range of hip motion was measured with a goniometer, indicating a decrease in flexion motion in patients with LBP compared to asymptomatic individuals. The researchers indicate the validity of hip joint assessment in people with LBP. The data obtained can provide information on diagnostic methods and treatment methods.
Reports from other researchers show that the occurrence of reduced hip flexion range of motion is associated with reduced functional capacity [25, 26].
In our study, a beneficial clinical effect was observed in both groups in the assessment range of motion of the hip joints immediately after the intervention. A significant increase in the result was noted in the study group: for the right limb by 15.3 points, for the left limb by 13 points; and in the control group, by 15 points and by 18 points, respectively. In the follow-up measurements, 1 and 3 months after the end of the therapy, a slight decrease in the results was noted in the study group, reaching a final improvement for the right limb by 12.3 points and for the left limb by 10 points. In the control group, however, a deterioration in the results was noted in the distant measurements; the effects were unstable. This is a surprising result because the patients performed a set of exercises. In the comparisons between the study group and the control group, statistically significant differences were observed (p < 0.05) in all measured time intervals for both lower limbs. Increasing the range of motion of the hip joints may improve functional performance in patients with LBP.
This article demonstrates that the results regarding improved hip range of motion are beneficial for patients with LBP. It is reasonable to suggest that decreased range of motion of hip movement may be one of the factors contributing to the development of LBP. The results of our research indicate the effectiveness of using the DN technique according to the FRSc in improving the efficiency of the patient with LBP. The best results were obtained immediately after the completion of the treatments, but the results at 1 and 3 months are also promising.
Our study did not assess the presence of a lumbosacral transitional vertebra (LSTV). This is a significant developmental anomaly that can lead to intervertebral disc degeneration (IVDD). Studies by Yu et al. [27] and Coskun Benlidayi et al. [28] demonstrated that the presence of LSTV is significantly associated with earlier development of IVDD and biomechanical changes in the lumbar spine. This anomaly may affect the distribution of forces acting on the intervertebral discs, leading to their overloading and accelerated degeneration, especially in the segments above the transitional vertebra.
Implications
Given the growing clinical use of DN according to the FRSc, it is worth continuing research on the effectiveness of this therapy based on other indicators and measurement tools to comprehensively assess the usefulness and effectiveness of this method. The preliminary results of the present study are promising, but they should be verified by other researchers to confirm the clinical usefulness of this method in patients with LBP. The DN method according to the FRSc can be used to provide therapeutic support to patients with LBP, improving functional capacity and quality of life.
Study limitations
A limitation of this study is the small number of patients; therefore, it would be worth continuing the project with a larger study sample and a longer follow-up period. In the future, it would also be worth expanding the methodological scope to include additional, objective measurement techniques. Standardization of intervention parameters (number of treatments, their frequency, and duration of a single application) is also recommended, which will enable a more consistent assessment of effectiveness. A significant limitation is the lack of assessment of the presence of the LSTV in imaging studies. This anomaly is related to the frequency and location of degenerative changes in the intervertebral discs; omitting this factor may affect the interpretation of the obtained results. Further studies involving a larger number of centers and independent research teams are recommended, which will enable validation of the obtained results and increase their reliability.