
Introduction
Use of vibrating tools at work often leads to development of the hand-arm vibration syndrome (HAVS). It manifests with vascular symptoms (occupational Raynaud’s disease), neurologic (carpal tunnel syndrome – CTS) and musculoskeletal symptoms (impaired grip strength, osteoarthritis, bone necrosis).
The HAVS has been reported in forestry and quarry workers, builders, carpenters, mechanics, dentists, and physiotherapists using ultrasonic therapy devices [1, 2]. Grinders, hammers, wrenches and saws pose the highest risk for developing HAVS in users.
The HAVS is more common in men than women (11 : 1) and affects 6–100% of exposed workers. In the United Kingdom the incidence was 113 new cases in 1993/1994 and 1009 in 2001/2002. In Australia only 3 cases were reported in 2000, but reporting is not mandatory there [1].
Kienböck’s disease is osteonecrosis of the lunate. Its incidence is not known. It was described by Robert Kienböck, a Viennese radiologist in 1910 [3]. He provided radiologic evidence for the entity. He recommended excision of the bone in case of severe pain and disability.
Case report
A 61-year-old non-smoker construction worker was referred to a rheumatologist because of suspected arthritis. On examination tenderness and swelling of the dorsal aspect of the right wrist (Fig. 1) were recorded without features of inflammation (Panel A). Flexion was restricted to 45º and extension to 40º. Phalen’s test was positive. The patient reported paresthesia in the right hand when working with a pneumatic drill. He reported no morning stiffness or Raynaud’s phenomenon. He had undergone surgery because of right CTS two years earlier. There were no other diseases in the medical history of the described patient.
Fig. 1
Swelling of the dorsal aspect of patient’s wrist (panel A). Magnetic resonance of the wrist: avascular necrosis of the lunate (red arrow, panel B) and scaphoid fracture (blue arrow).
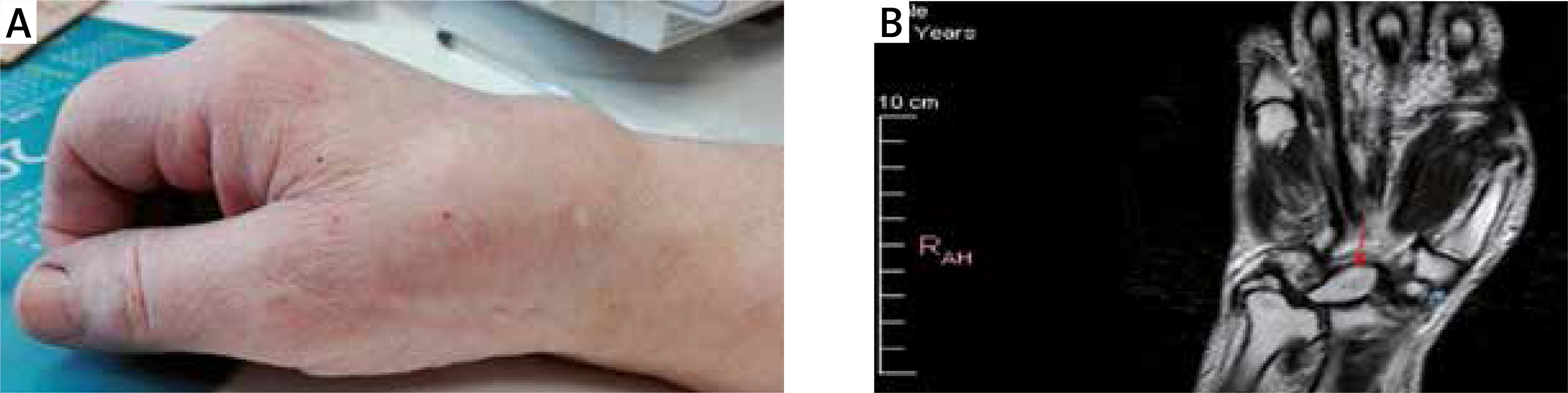
Rheumatoid factor was negative, C-reactive protein 0.2 mg/l, uric acid 4.7 mg/dl, fasting glucose was 99 mg/dl, urine analysis was within the normal range, antinuclear antibodies were not detected. In magnetic resonance imaging (MRI) avascular necrosis of the lunate was diagnosed (indicated by a red arrow in panel B) and scaphoid fracture (indicated by a blue arrow). Kienböck’s disease was diagnosed.
The patient refused surgery and as the basic treatment received non-steroidal anti-inflammatory drugs (NSAIDs). The diagnosis of Kienböck’s disease may be understood as a consequence of HAVS.
Discussion
Diagnosis of HAVS is based on exposure history and symptoms, examination plus specific tests. Neurological symptoms are associated with peripheral neuropathy, with tingling, numbness and finger pain, but it needs to be distinguished from peripheral neuropathy in other diseases such as diabetes, autoimmune diseases, viral infections (herpes Zoster, hepatitis B or C, Epstein-Barr virus) infections, but also alcohol abuse, drugs (especially chemotherapeutic drugs), vitamin deficiency (vitamin B1, B6, B12 and vitamin E).
In the course of the disease reduced motor coordination and grip strength are observed. One of the most important vascular symptom of HAVS is Raynaud’s phenomenon with local finger blanching caused by vasospasm of the skin venules. In addition to the term Raynaud’s syndrome also term vibration white finger (VWF) is sometimes used to describe vascular disturbances caused by vibrations.
Musculoskeletal symptoms may include osteoarthritis, carpal tunnel syndrome, bone cysts, tendinopathies, and even avascular bone necrosis [1].
Physical tests used for diagnosis of HAVS are the cold provocation test, Allen’s test, Doppler ultrasound and thermography. In diagnosis of neurological symptoms, the light touch test, pin prick, thermal threshold testing, vibration perception threshold, two point discrimination test, nerve conduction study, electromyography, Tinel’s test, and Phalen’s test are used. Musculoskeletal symptoms are assessed by grip and pinch strength tests, X-ray, ultrasonography or magnetic resonance. During the diagnostic course the exclusion of other comorbidities is necessary.
Laboratory tests such as erythrocyte sedimentation rate, blood viscosity, uric acid, glucose, rheumatoid factor, antinuclear antibodies, cryoglobulins, and serum protein electrophoresis should be performed, and also the general urine and urine sediment test is necessary to exclude proteinuria and glycosuria. If a male patient working with vibrating tools presents with carpal tunnel syndrome (CTS), it is important to consider a diagnosis of HAVS [1].
Kienböck’s disease is rarely diagnosed by a rheumatologist. However, we should be aware of possible causes of this disease. The extraosseous vascularity of the lunar bone is physiologically profuse through two or three dorsal and three to four volar vessels feeding dorsal and volar capsular plexuses. The intraosseous vascularity is formed by one or three consistent patterns with anastomoses of dorsal and volar vessels. The vascular patterns support the theory of compression fracture from repeated trauma as the most likely cause of Kienböck’s disease [4].
Hereditary factors are also considered likely in the pathogenesis of Kienböck’s disease. Templeman and Engber [5] described familial occurrence of avascular necrosis of the lunate in a mother and her daughter manifesting with dorsal wrist discomfort, dorsal swelling and flexion restricted to 55º and extension to 35º in both cases.
Hungarian authors reported vascular, neurological and osteoarticular changes due to HAVS in caisson miners [6]. It might be due to use of heavy vibrating tools and gas embolism due to rapid change in the atmospheric pressure (caisson disease). Cases of aseptic osteonecrosis of the lunate caused by repeated microtrauma were described in employees in the mining and metallurgic industry by Romanian authors [7].
Decades after Kienböck described avascular necrosis of the lunate, the options of treatment have changed to be: immobilization for three months (in stage I with normal radiographs), radius shortening osteotomy and ulnar lengthening in case of negative ulnar variance (in stage II with lunate sclerosis) or direct revascularization in case of positive ulnar variance (in stage III with lunate collapse), scaphotrapeziotrapezoid or scaphocapitate fusion (stage IIIB) and proximal-row carpectomy or wrist arthrodesis (in stage IV with severe lunate collapse with intra-articular degenerative changes) [8].
Stahl et al. [9] systematically reviewed factors affecting development of Kienböck’s disease. The most common etiological factors of the disease are: negative ulnar variance, primary arterial ischemia of the lunate, trauma, embolism and hand-arm vibration [5, 9]. However, according to the International Labor Organization Kienböck’s disease does not comply with criteria determining occupational diseases. At the same time, the authors emphasize that HAVS is a risk factor for development of Kienböck’s disease.
Interestingly, there is evidence that low-magnitude whole-body vibration therapy can provide a significant improvement in reducing bone loss in the lumbar spine in postmenopausal women [10]. The high-frequency but low-magnitude vibration positively influences bone formation and, what is important, in treatment of osteoporosis decreasing bone resorption [11]. This anabolic effect is attributed to the effect of this kind of vibrations on osteocytes, tendons, and muscles.
Anabolic effects of low-intensity mechanical signals on bone may be induced indirectly via extra-skeletal tissues. Enhanced muscle strength, size, and performance were observed in humans and animals following vibration, possibly due to increased neuromuscular efficiency. Also vibration enhances expression of anabolic genes in tendons [11, 12].
Paget-Schroetter syndrome in which primary thrombosis of the axillary/subclavian vein at the costoclavicular junction occurs, can also be a complication of vibration. It is a rare disease, but it should also be taken into account in differentiating pain, swelling, and weakness in the upper limb in a person who works physically with mechanical devices that cause vibrations [13].
Conclusions
Work with vibrating tools may lead to HAVS, which can manifest with vascular, neurological and musculoskeletal symptoms including bone necrosis. The hand-arm vibration syndrome is also a risk factor for developing avascular necrosis such as Kienböck’s disease, as was described in the present case.