
Introduction
In late 2019, a new infectious disease, known as coronavirus disease 2019 (COVID-19), occurred in the Wuhan province of China, which caused a novel acute respiratory syndrome and severe pneumonia [1, 2]. The rapid transmission of the causative virus and the unpredictable and aggressive behavior led the World Health Organization (WHO) to refer to COVID 19 as a 21st century disaster [3].
Angiotensin-converting enzyme 2 (ACE2) receptors are expressed on the host cell’s surface. By binding to these receptors, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus can easily infect multiple organs and cause anarchy in immune system responses [4].
Moreover, the primary investigations showed that patients with underlying medical conditions and those who received immunosuppressive agents are more likely to develop COVID-19 [5, 6].
Among different diseases related to the immune response, rheumatic diseases are the most common chronic inflammatory diseases affecting various organs with multiple systematic symptoms. Despite physical complications, pain, and the higher risk for developing simultaneously other complications such as cardiovascular diseases [7], one of the main concerns over rheumatic diseases is the side effects of immunosuppressive therapy [8].
Glucocorticosteroids (GCs), disease-modifying antirheumatic drugs (DMARDs) such as methotrexate (MTX), anti-tumor necrosis factors (anti-TNFs), and rituximab (RTX) are among the most common medications that can result in unprecedented responses in the treatment of rheumatic patients in Iran [9].
The increased risk for tuberculosis, hepatitis B, and hepatitis C related to GCs and DMARDs was so significant that many studies suggested strict screening and prophylactic protocols in those patients [10–12].
This correlation became a major issue during the COVID-19 pandemic. No consensus exists yet on whether or not DMARDs can elevate the risk of developing COVID-19. However, the European Alliance of Associations for Rheumatology (EULAR) and the American College of Rheumatology (ACR) at the beginning of the pandemic suggested that it was appropriate to discontinue some of the medications in this era [13, 14].
Avouac et al. [15] reported that RTX could elevate the risk of COVID-19 incidence and mortality 1.32-fold for rheumatic patients.
On the other hand, some evidence showed that the application of such medications could be promising for the outcome of the patients. Monti et al. [16] evaluated the influence of biologic DMARDs (bDMARDs) and conventional DMARDs (cDMARDs) on COVID-19 for a month and reported that these drugs have no impact on severe complications of COVID-19.
In another study, Tursi et al. [17] suggested that anti-TNFs could attenuate cytokine storm risk in patients with COVID-19 respiratory complications. Several studies also claimed the advantages or protective effects of hydroxychloroquine and anti-inflammatory drugs for rheumatic patients infected by the SARS-CoV-2 virus [8, 18].
Although multiple lines of evidence have evaluated the advantages and disadvantages of DMARDs and other immunosuppressive agents with respect to the incidence of COVID-19 in patients with rheumatic diseases, this association is still unclear.
The aim of the present study was thus to evaluate the correlation between DMARDs therapy and the risk of developing COVID-19 in rheumatic patients.
Material and methods
Patient collection
This longitudinal-analytical study was conducted on rheumatic patients who were previously, or at the beginning of the study, registered with the Rheumatic Diseases Research Center of Mashhad University of Medical Sciences, Mashhad, Iran.
Patients who were diagnosed according to the disease-related ACR/EULAR criteria and clinical and laboratory symptoms related to diseases including rheumatoid arthritis (RA), seronegative spondylarthritis (ankylosing spondylitis, psoriatic arthritis, reactive arthritis, and inflammatory bowel disease), Behçet’s disease, granulomatosis with polyangiitis, and polyarteritis nodosa vasculitis were chosen from the beginning of the first peak until the end of the second peak of the pandemic in Iran (February to July 2020).
All selected patients were over 18 years old. Patients with other rheumatic diseases such as lupus erythematosus, polymyositis/dermatomyositis, or systemic sclerosis were excluded from the study due to lower frequency of prescription during the pandemic or no approval protocol for available bDMARDs in our country.
For a few patients (28) who participated in the study by telephone contact, the email of the informed consent was sent, and most of them underwent at least one face-to-face visit during the follow-up. Patients filled in a checklist on their demographic data, including age, gender, occupation, the number of family members, the presence of underlying diseases, and medications.
Moreover, a checklist was completed by patients regarding their compliance with health protocols/social distance during the outbreak of COVID-19. High-risk jobs are defined as all healthcare staff and employees working in crowded indoor workplaces such as factory workers who did not include teleworking during the lockdowns.
COVID-19 diagnosis
From the beginning of the first peak of the COVID-19 pandemic in Iran, 512 mentioned rheumatic patients who were either previously registered with this center, hospitalized in the COVID departments of our university hospitals, or patients contacted by phone according to telemedicine follow-ups were selected to participate in this study consecutively.
Those patients who did not respond to our phone calls or refused to participate in the study were excluded (32 patients). It should be noted that all the attendees were treated with cDMARDs ± GCs, with or without bDMARDs.
This research was conducted at the beginning of the outbreak and at that time, we followed our regional Ministry of Health Guidelines for diagnosis; therefore, our guideline used highly suggestive clinical symptoms and exposure in addition to paraclinical factors such as a chest X-ray (CXR) or computed tomography (CT) scan result, lymphopenia and C-reactive protein (CRP) with or without obtaining a COVID-19 PCR to detect the COVID-19 cases.
At the time of the current study COVID-19 PCR was not available routinely (it was used only for patients admitted to the hospital at the beginning of the first peak). The physicians recorded the clinical symptoms such as fever, sore throat, myalgia, diarrhea, pharyngitis, cough, and anosmia.
In symptomatic patients, according to the results of the PCR, if the patient underwent the test, and the lung CT scan or CXR, the SARS-CoV-2 virus-infected patients were categorized into three main groups as follows.
“Definite COVID-19 patients” were those with positive PCR test results; “probable COVID-19 patients” were patients with highly suggestive symptoms with positive lung imaging who did not undergo COVID-19 PCR due to a shortage of the test, and “suspected COVID-19 patients” were those who had suggestive symptoms or close contacts without any information about the lung CT/CXR or PCR results due to uncooperating of the patient.
Given the low number of “probable COVID-19 patients”, we considered them definite ones.
All patients with COVID-19 infections should have spent 14 days in quarantine. Participants were followed up by visits or by calling them or their first-degree relatives until the end of the second peak of COVID-19.
Statistical analysis
All the statistical analyses were done with SPSS 25.0 software and the GraphPad Prism software. The χ2 test and Fisher’s exact test were used to evaluate the relationship between the demographic features of the patients, type of treatments, and adherence to the health protocols and the incidence and the severity of COVID-19 in rheumatic patients.
The possible correlation between the aforementioned factors and the COVID-19 incidence rate among patients was investigated using regression analysis. Probability values less than 0.05 were regarded as statistically significant.
Results
Patients
Five hundred twelve patients with selected rheumatic diseases with a median disease duration of 7.16 ±6.95 years entered the study consecutively. Three hundred fifty-two patients (68%) had RA, 60 patients (11.7%) suffered from psoriatic arthritis, and 41 patients (8%) had ankylosing spondylitis.
Other diseases included Behçet’s disease (26 patients; 5.1%), granulomatosis with polyangiitis 23 patients; 4.5%), IBD-related arthritis (5 patients; 1%), and eosinophilic granulomatosis with polyangiitis (3; 0.6%). Notably, 0.4% of the patients (2 out of 512) showed simultaneous symptoms of ankylosing spondylitis and Behçet’s disease or RA and psoriatic arthritis.
Like other autoimmune diseases, most patients (76.76%) were female. Only in IBD, ankylosing spondylitis, and granulomatosis with polyangiitis did the percentage of men exceed that of women. Three hundred eighty out of 512 patients did not have any other underlying diseases, while 132 patients suffered from hypertension (14.1%) and diabetes (5.5%), with rheumatic disease.
Three hundred nine patients (60.4%) were treated with cDMARDs, 192 patients (37.5%) received both bDMARDs and cDMARDs, while 11 patients (2.1%) discontinued their treatment before the COVID-19 pandemic. Notably, 87.2% of patients with bDMARD were treated with anti-TNF, whereas 12.8% received RTX. In the cDMARDs group, patients were treated with MTX (about 7.5 mg/week), cyclophosphamide, hydroxychloroquine, sulfasalazine, azathioprine, and mycophenolate mofetil.
Moreover, along with DMARDs, 357 patients were also treated with prednisolone (less or more than 10 mg/day). After the first COVID-19 outbreak, 30 patients in our study stopped their medications; among them, 11 patients made this decision under the supervision of a doctor, and 19 patients arbitrarily stopped using DMARDs.
From the first peek of the COVID-19 pandemic in Iran, all studied rheumatic patients who were regularly referred to the hospital and health care centers were available by telephone contacts. They were followed up thoroughly for development of COVID-19 until the end of the second peak. All patients were also asked for detailed COVID-19 health protocol guidance, such as staying at a safe social distance, washing hands, and wearing masks.
Prevalence of COVID-19 among rheumatic patients
Our results showed that among 512 previously rheumatic patients, 154 complained of COVID-19-related symptoms. Among them, 88 patients were “definite COVID-19 patients”.
This group of definite patients included patients with only positive PCR (n = 34, 19.9%) without any lung involvement in imaging and patients with both positive PCR and lung involvement in imaging (n = 54, 64.4%). Moreover, “probable COVID-19 patients” (n = 14, 2.7%) included patients with positive COVID-19 related lung imaging who did not undergo COVID-19 PCR.
In line with our regional guideline in the study, we put the probable patients in the COVID-19 positive group for statistical analysis. In total, 102 patients were selected as documented coronavirus-infected patients. “Suspected COVID-19 patients” included 52 patients (10.2%) who were health care workers or patients’ relatives with close contact with COVID-19 patients and common cold symptoms who did not test for PCR or lung imaging, whom we did not consider as infected patients (Table I).
Table I
Symptoms in COVID-19-infected rheumatic patients*
In total (19.9–20%) of our patients were diagnosed as SARS-CoV-2 definite patients. The median age of COVID-infected rheumatic patients and non-infected subjects was 49.1 ±12.9 and 47.9 ±13.2, respectively, which was statistically insignificant (p = 0.4). Fever (97.7%), myalgia (97.7%), and headache (63.6%) were the most common symptoms of COVID-19 in rheumatic patients. Twenty-three point nine percent of COVID-19-infected patients with RA were hospitalized because of respiratory symptoms, and only one patient with granulomatosis with polyangiitis treated with prednisolone (> 10 mg/day) died in the ICU (Table I).
Correlation between COVID-19 infection and the type of rheumatic disease
Based on the previous findings, we aimed to evaluate whether there is a correlation between various types of rheumatic diseases and the frequency of COVID-19 infection. Our results showed that the frequency of COVID-19 between different groups of rheumatic patients was the same.
The number of patients in each disease and the number and percent of COVID-19 infected cases are as follows: RA (60/352 – 17%), psoriatic arthritis: (10/60 – 9.8%), ankylosing spondylitis: (11/41 – 10.8%), Behçet’s disease: (9/26 – 8.8%), granulomatosis with polyangiitis: (10/23 – 9.8%), IBD-related SPA: (5/1 – 1%), eosinophilic granulomatosis with polyangiitis: (3/1 – 1%). In 2 patients with simultaneous symptoms of both ankylosing spondylitis and Behçet’s disease or RA and psoriatic arthritis, no case of COVID-19 was reported. There was no significant relationship between the frequency of COVID-19 infection and the type of rheumatic diseases (p = 0.45, χ2 test).
Association between demographic characteristics of rheumatic patients and COVID-19 infection
Proposing the vulnerability of rheumatic patients to the SARS-CoV-2 virus, it was of particular interest to evaluate the correlation between the risk of contracting COVID-19 and demographic features of the patients. As presented in Table II, the χ2 test results indicated that the incidence rate of COVID-19 was significantly higher in women than men (p = 0.012), which could be due to the higher frequency of the rheumatic diseases in females.
Table II
Association between demographic features of rheumatic patients and COVID-19 infection
| Factors | COVID-19 infection | p-value* | |
|---|---|---|---|
| No Frequency (%) | Yes Frequency (%) | ||
| Gender | |||
| Female | 322 (78.5) | 68 (66.7) | 0.012 |
| Male | 88 (21.5) | 34 (33.3) | |
| Number of family members | |||
| ≤ 3 | 226 (55.1) | 48 (47.1) | 0.144 |
| > 3 | 184 (44.9) | 54 (52.9) | |
| Occupation status | |||
| Employed | 99 (24.1) | 33 (32.4) | 0.180 |
| Housewife | 264 (64.4) | 56 (54.9) | |
| Unemployed | 47 (11.5) | 13 (12.7) | |
| Type of occupation | |||
| Workplace | 78 (78) | 28 (87.5) | 0.773 |
| Telecommuting | 22 (22) | 4 (12.5) | |
| Type of job | |||
| High risk** | 35 (35.4) | 10 (30.3) | 0.596 |
| Low risk | 64 (64.6) | 23 (69.7) | |
| Smoking | 16 (3.9) | 3 (2.9) | 0.643 |
| Addiction | 17 (4.2) | 3 (2.9) | 0.566 |
| Underlying disease | |||
| No disease | 309 (75.6) | 71 (69.6) | 0.058 |
| Diabetes | 18 | 9 | |
| Blood pressure | 58 | 14 | |
| Chronic renal failure | 1 | 0 | |
| Malignancy | 2 | 0 | |
| Diabetes and stroke | 0 | 1 | |
| Diabetes and blood pressure | 20 | 5 | |
| Chronic renal failure and blood pressure | 1 | 0 | |
| Diabetes, blood pressure and chronic renal failure | 0 | 1 | |
| Drugs | |||
| Methotrexate | |||
| Yes | 305 (74.4%) | 63 (61.8%) | 0.011 |
| No | 105 (25.6%) | 39 (38.2%) | |
| Sulfasalazine | |||
| Yes | 87 (21.2) | 16 (15.7) | 0.21 |
| No | 323 (78.8) | 86 (84.3) | |
| Hydroxychloroquine | |||
| Yes | 98 (23.9) | 10 (9.8) | 0.002 |
| No | 312 (76.1) | 56 (54.9) | |
| Cyclophosphamide | |||
| Yes | 4 (1) | 4 (3.9) | 0.032 |
| No | 406 (99) | 98 (96.1) | |
| Azathioprine | |||
| Yes | 10 (2.4) | 5 (4.9) | 0.18 |
| No | 400 (97.6) | 97 (95.1) | |
| Mycophenolate mofetil | |||
| Yes | 1 (0.2) | 1 (1) | 0.26 |
| No | 409 (99.8) | 101 (99) | |
| Biologic DMARDs (anti-TNFs and RTX) | |||
| Yes | 148 (37) | 44 (43.5) | 0.31 |
| No | 252 (63) | 57 (55.5) | |
Unlike gender, other demographic features such as occupation, number of family members, smoking, and addiction had no significant effect on the individuals’ susceptibility to the SARS-CoV-2 virus (p > 0.05). No relationship was observed between COVID-19 infection and underlying diseases, such as diabetes, high blood pressure, renal failure, and malignancies (p = 0.058) (Table II).
Association between adherence to the health protocol and COVID-19 prevention guidelines among rheumatic patients
Since the COVID-19 outbreak, following health protocols and guidelines, such as social distancing, wearing a mask, and practicing hand hygiene, was claimed to be the only way to control the transmission of the virus at the time of the study [19].
The influence of the health protocols on the prevalence rate of COVID-19 was explored among patients. A significant association was detected between wearing masks, hand hygiene, and disease incidence. The results showed that 97.8% of patients without COVID-19 used masks, but this percentage for the SARS-CoV-2-infected patients dropped to 93.1% (p = 0.015).
Accordingly, the same results were obtained for hands hygiene, as 98.8% of rheumatic patients who regularly washed their hands were not infected with SARS-CoV-2, whereas only 95.1% of patients with COVID-19 adhered to hand hygiene protocols (p = 0.016). There was no apparent relationship between social distancing and other health protocols and COVID-19 (p = 0.410).
Association between the treatment strategy and COVID-19 infection
Tables II and III show the frequency of prescribing each DMARD and global bDMARDs and cDMARDs in all patients and the hospitalized subjects. One hundred ninety-two patients (37.5%) treated with bDMARDs and cDMARDs and 11 (2.1%) patients stopped bDMARD therapy independently or with physicians’ consultation.
Table III
Association between biologic/conventional disease-modifying antirheumatic drugs and incidence of COVID-19 infection in rheumatic patients
A χ2 test was utilized to evaluate whether the combination of bDMARDs and cDMARDs increases the risk of COVID-19 infection. Table III presents no association between the type of the groups mentioned above and the COVID-19 infection among patients, irrespective of the disease types.
However, the test was carried out for each disease type to ensure that using DMARDs could not make rheumatic patients more vulnerable to the SARS-CoV-2 virus. In agreement with the previous results, adding bDMARDs to cDMARDs could not alter the susceptibility of the patients to COVID-19 (Table III).
As regards cDMARDs, MTX significantly increased and hydroxychloroquine significantly decreased the chance of COVID-19 infection in our patients. In a few patients treated with cyclophosphamide, the risk of infection and death was increased (Table II).
In bDMARD-treated patients, 177 received anti-TNFs, and 26 received RTX. Thirty-six (80%) anti-TNF treated individuals and 9 (20%) RTX treated patients got infected with COVID-19.
On the other hand, 141 (89.2%) anti-TNF and 17 (10.8%) RTX treated individuals were COVID-19 free; therefore, the type of those biologic therapies did not affect the risk of COVID-19 infection (p = 0.1, χ2 test).
Moreover, the hospitalization rate was also not different between those biologic therapies (p = 0.3, χ2 test). Regarding GC therapy: 357 (69.7%) participants were treated with GCs in different doses 341 (95.5%) less than 10 mg/day and 16 (4.5%) more than 10 mg/day. Sixty-two and a half percent of patients treated with more than 10 mg/day prednisolone got infected with COVID-19 while 17.5% of patients treated with less than 10 mg/day got infected with coronavirus (p = 0.0001, χ2 test).
Moreover, the number of admitted patients in the group of patients treated with more than 10 mg/day prednisolone was significantly higher (70%) than in the group of patients treated with smaller doses (21.6%) (p = 0.005, χ2 test).
The only patient who died received more than 10 mg/day of prednisolone. Regarding MTX therapy, in our study 117 patients (31/8) were treated with less than 7.5 mg/week and 251 (68/2) were treated with more than that dose.
Conventional and biologic disease-modifying antirheumatic drugs, the risk of hospitalization of infected patients with COVID-19
In this research, the frequency rate of COVID-19 infection in 512 rheumatic patients was 19.9%. The rate of hospitalization in our COVID-19 infected patients was 23.9%. The mortality rate was also estimated to be 0.19%, which occurred in one patient with granulomatosis with polyangiitis under treatment with high doses of GC and cyclophosphamide.
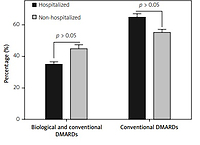
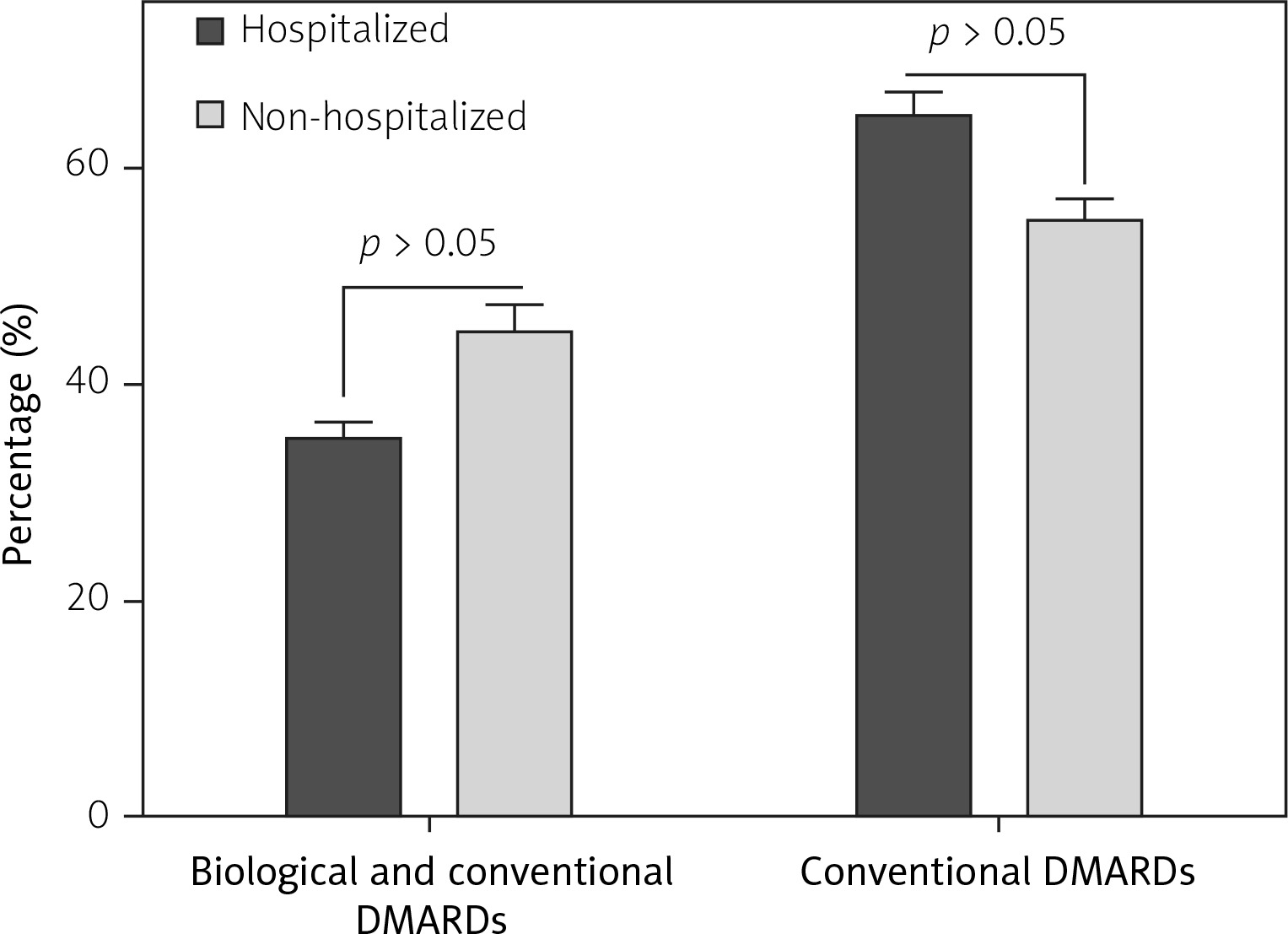
Sixty-five percent of hospitalized patients were only treated with cDMARDs, whereas the remaining 35% received both bDMARDs and cDMARDs. Similarly, 55.2% of outpatient cases were only treated with cDMARDs, and 44.8% received bDMARDs and cDMARDs (p = 0.46, χ2 test). Therefore, DMARDs did not affect the COVID-19 hospitalization (Fig. 1).
Fig. 1
Influence of biologic and conventional disease-modifying antirheumatic drugs on hospitalization of rheumatic patients infected with SARS-CoV-2. As presented, neither biologic nor conventional DMARDs significantly altered the hospitalization rate of rheumatic patients. Values are reported as mean ±SD of three independent experiments. Statistical significance was defined as p < 0.05.
As we mentioned above, the prednisolone therapy and its dosage increased the risk of admission of our patients due to COVID-19 infection. Only one of the study patients died, who had a known case of granulomatosis with polyangiitis and was treated with cyclophosphamide and prednisolone more than 10 mg.
Regression analysis on the important initial factors that influenced COVID-19 infection in the rheumatic patients
Based on the results obtained in the present study and cumulative data, the statistically significant factors that influenced COVID-19 infection in rheumatic patients were gender, adherence to health protocol, including wearing masks, hand hygiene, and some cDMARDs (MTX, hydroxychloroquine, and cyclophosphamide), and prednisolone dosage.
In the next step, the regression correlation coefficient test was employed. Among the mentioned factors, prednisolone (> 10 mg/day) was associated with up to 5-fold increased risk of COVID-19 development (OR = 4.7, p = 0.008) (Table IV).
Table IV
Regression analysis of important risk factors for COVID-19 infection in rheumatic patients based on initial results
Moreover, the incidence risk of COVID-19 was approximately 40% lower in the patients who were treated with hydroxychloroquine (OR = 0.4, p = 0.022). The resulting data also indicated that other factors such as gender, health protocols, and type of DMARDs did not significantly influence the COVID-19 in rheumatic patients.
Comparison of demographic and related disease data between suspected and definite groups of COVID-19
As mentioned above, 102 definite and 52 suspected patients, according to the local guide line definitions, were diagnosed. Type of rheumatic diseases showed no significant difference between the two groups. Female gender was more common in the suspected group (n = 44) than the definite one (n = 68) (p = 0.01, χ2 test).
There was no significant difference in the adherence to the COVID-19 infection prevention guidelines between the two groups, including social distancing, hand hygiene and wearing a mask, and the frequency of underlying diseases. Three smokers were found in the definite group and one in the suspected group.
Thirty-six definite patients and 21 suspected ones received anti-TNF therapy, nine definite and three suspected patients received RTX, there was no significant difference between two groups according to bDMARDs (p = 0.3, χ2 test), and no difference between the groups in the number of patients receiving biologics or the type of the drugs.
In addition, the frequency of cDMARDs did not differ significantly between the two groups (p = 0.45, χ2 test). Dose of the medication and arterial hypertension, number of patients treated with prednisolone were not significantly different between the two groups (p = 0.24). There was no significant difference in bDMARDs withdrawal between the two groups (p = 0.4 Fisher’s exact test). All suspected patients complained of fever, myalgia, and sore throat.
Discussion
From the first case of COVID-19 infection in 2019, patients with underlying medical conditions, such as diabetes, cardiovascular diseases, cancers, and arterial hypertension, had a more significant health concern. From the beginning, there was the hypothesis that these patients were more likely to be infected and may have a more severe course of COVID-19 than the general population [20–22].
Autoimmune patients are also suspected at higher risk for developing COVID-19 as well. The present research was designed to examine the correlation of the application of immunosuppressive agents, including prednisolone and bDMARDs and cDMARDs, with the incidence of COVID-19 infection in rheumatic patients during the first two COVID-19 outbreaks.
The main results of our study were as follows:
The frequency of COVID-19 infection in 512 rheumatic patients with different types of diseases was 19.9%. The rate of hospitalization in our COVID-19 infected patients was 23.9%. The mortality rate was also estimated to be 0.19%, which occurred in one patient with granulomatosis with polyangiitis.
There was no correlation between the type of rheumatic diseases and COVID-19 infection.
Treating with anti-TNFs and RTX in addition to cDMARDs did not increase the risk of COVID-19 infection and hospitalization in our patients.
Glucocorticosteroid therapy, especially with doses of more than 10 mg/day prednisolone, increases the risk of COVID-19 infection and hospitalization.
Methotrexate therapy significantly raised the number of COVID-19 infected patients.
Hydroxychloroquine significantly reduced the number of COVID-19 infected patients.
Most of our patients, specially bDMARDs treated individuals, adhered to health protocols due to insight into immunosuppression and increased risk of infections.
Biological DMARDs did not increase the mortality rate due to COVID-19 infection in our patients.
A recent meta-analysis of more than 300,000 autoimmune patients revealed that the incidence risk of COVID-19 infection is twice as high in patients with chronic autoimmune diseases compared with their healthy counterparts [23].
Among autoimmune diseases, the results for the influence of rheumatic diseases on the susceptibility of patients to the SARS-CoV-2 virus are still controversial. Although some studies have claimed that the COVID-19 incidence rate might not be higher in rheumatic patients, it should be remembered that immunosuppressive agents such as DMARDs and GCs could expose the patients to a higher risk of viral infections [24].
Despite the ameliorating effects on disease symptoms, immunosuppressive agents such as anti-TNF and rituximab increase the risk of bacterial and viral infection in the patients, putting the application of such drugs during a pandemic under debate.
The correlation between rheumatic disease and the incidence risk of COVID-19 has been examined in different studies and yielded inconsistent results. While a previous report indicated that the incidence of COVID-19 and the hospitalization rate in inflammatory arthritis are 7.2% and 9.3%, respectively [25], other studies failed to detect a correlation between these two diseases.
Conticini et al. [26] reported that of 895 rheumatic patients, only two patients were infected by SARS-CoV-2. In another study, Favalli et al. [27] estimated that in 2050 patients with inflammatory arthritis, definite and suspected COVID-19 rates were 1.1% and 1.4%, respectively, suggesting that rheumatic diseases could not increase the incidence risk of COVID-19 development in the individuals.
Gianfrancesco et al. [28] reported that 46% of rheumatic patients with SARS-CoV-2 infection were hospitalized, and about 9% of these patients lost their lives. Strangfeld et al. [29] also reported the mortality rate of 10.5% for COVID-19 in rheumatic patients, which was significantly higher than the rate observed in the current study.
Based on the previous findings and given the fact that about 97% of the participants in the present study adhered to the health protocols, the COVID-19 frequency rate of 19.9% indicated that rheumatic disease could probably act as a risk factor capable of promoting the disease even by exposure to a low viral load.
Additionally, since many studies have emphasized the devastating effects of bDMARDs on the outcome of COVID-19 infection, rheumatic patients receiving this type of drug were more prone to adhering to hygiene protocols or were more under medical supervision. The lower COVID-19 incidence rate in our patients can be attributed to the precautions taken by both the patient and the physician.
Besides the underlying disease, individual characteristics seem to be involved in developing COVID-19 disease. It has been claimed that there is a gender-based difference in the COVID-19 severity among the individuals as male patients have a higher mortality rate and disease severity, which could be due to the influence of androgens and ACE2 receptor presentations in the lungs [30].
In this research, however, the prevalence rate of COVID-19 infection was higher in women, which can be attributed to the higher prevalence of rheumatic diseases in females – in addition to gender, wearing masks with standard health protocols, such as sanitizing were other influential factors that could determine the severity of COVID-19 infection in patients with rheumatic diseases.
It is worth mentioning that although the incidence rate of COVID-19 seems to be higher in RA (17%), ankylosing spondylitis (12.5%), and granulomatosis with polyangiitis (11.4%), they showed no significant difference with other groups.
Neither smoking nor addiction was associated with increased risk of developing COVID-19 in our rheumatic patients. However, the small number of addict and smoker patients makes this result inconclusive. As most of our patients were female, the number of smokers and addicts was deficient. A study showed that the mortality rate of COVID-19 was lower in smoker patients; also, it had limitations [31].
The application of immune-modulatory agents was another criterion that has been enumerated in determining the susceptibility of the patients to viral infections. One study conducted on MS patients found that COVID-19 development was significantly higher in patients who received ocrelizumab, an antiCD20 therapy targeting B lymphocytes [32].
It was of particular interest to evaluate whether the type of treatment in rheumatic patients could affect their susceptibility to COVID-19. Interestingly, although the type of DMARDs and the incidence rate of COVID-19 in patients with rheumatic diseases were not significantly correlated, it seems that those treated with cDMARDs are at higher risk for developing COVID-19.
Moreover, in our study, treatment with cDMARDs was twice as frequent as that with bDMARDs in hospitalized patients. It is notable that cDMARDs are used much more frequently than bDMARDs. Among cDMARDs, MTX, hydroxychloroquine, and cyclophosphamide appear to significantly affect the incidence and the severity of COVID-19 in these patients.
Also, the sample size of patients treated with cyclophosphamide in this study was too small to be conclusive. The resulting data also indicated that patients who received hydroxychloroquine had a 40% lower chance of COVID-19 infection. In line with our findings, Akiyama et al. [23] stated that unlike bDMARDs, such as anti-TNF, cDMARDs could increase the severity and the mortality rate of COVID-19 patients.
Another study also indicated that bDMARDs could reduce the incidence rate of COVID-19 infection 0.47-fold [27]. The deteriorating impact of cDMARDs on COVID-19 progression has been reported in several studies.
However, in agreement with our findings, Migkos et al. [25] reported that hydroxychloroquine had no adverse effect on the intensity of COVID-19 in patients with rheumatic diseases.
The more decisive influence of bDMARDs on the severity of COVID-19 could be due to the suppressive effect of these drugs on the COVID-19-induced cytokine storm [18]. There are conflicting data on the prophylactic and treatment role of hydroxychloroquine, especially during the initial outbreaks without enough knowledge and access to vaccination.
A meta-analysis revealed that the prevalence rate of COVID-19 was strikingly lower in the individuals who were treated with hydroxychloroquine prior to exposure to the SARS-CoV-2 virus. Apart from the protective effects of hydroxychloroquine, this meta-analysis also provided more information on the safety of weekly administration of the drug and proposed starting universal vaccination [33].
Hydroxychloroquine was the mainstay of local treatment guidelines before vaccination in our country. As regards MTX, the fact that most of our patients were treated with high doses of this drug (more than 7.5 mg/week) may be due to more disease activity or discontinuation of bDMARDs.
Although it is hypothesized that MTX may act protectively against COVID-19 infection due to increased adenosine formation and decreased ACE2 lung receptors [34], our study showed that in higher doses combination DMARDs therapy or disease activity does not support this hypothesis. Moreover, the large number of patients treated with MTX in this study (368 patients) increases the power of our findings.
Apart from DMARDs, prednisolone is one of the essential GCs used in treating rheumatic patients. Several studies have scrutinized the influence of prednisolone on the incidence of COVID-19. In this regard, Strangfeld et al. [29] found that prednisolone at a dosage > 10 mg/day was associated with elevated risk of hospitalization due to COVID-19 infection in rheumatic patients.
In another study on 600 rheumatic patients, Gianfrancesco et al. [28] declared that high doses of prednisolone could increase the hospitalization risk 2-fold. In agreement with these studies, here, prednisolone at a dosage higher than 10 mg/day led to a 5-fold increase in the incidence rate of COVID-19 in our patients. Second, COVID-19 patients who were treated with a higher dosage of this GC were more prone to be hospitalized.
Regression analysis showed that the GC is a free risk factor for this infection independent of other risk factors for COVID-19 infection, such as other DMARD therapies.
This influence could be discussed from two perspectives. First, it is well-established that prednisolone can remarkably inhibit the secretion of stimulatory cytokines by halting the activity of the nuclear factor κB signaling axis [35]. Moreover, by suppressing the effect of cytotoxic T cells, this GC could stop one of the most important arms of the immune system against viral infections [36].
Additionally, patients with more severe underlying diseases might require a greater concentration of the drug. Indeed, the severity of the underlying disease probably increases the patients’ vulnerability to the SARS-CoV-2 virus. The results from this study indicated that the use of drugs such as prednisolone could increase the prevalence risk of COVID-19 in patients with rheumatic diseases. However, we know that dexamethasone plays a critical therapeutic role in the cytokine storm of COVID-19 infection [29].
Study limitations
Some limitations of this study are as follows:
Due to the fear of COVID-19 infection, some patients did not respond to our follow-up appointment and were reluctant to refer to the hospital or health care centers, and did not participate in the study.
On the other hand, the answer of the COVID-19-infected patients to the questions on observing the health protocols and guidelines about the higher risk of infection might be biased.
The follow-up plan and completing the checklist made the patients more alert about the risk of COVID-19 infection, and it may affect their behaviors and protecting lifestyle during the outbreaks.
The lack of PCR test for COVID-19 screening during the first episodes of the outbreak led to missing a significant percentage of mildly infected patients in our research, and therefore, the results may be applicable for more symptomatic patients.
Conclusions
This study revealed that during the first and second COVID-19 outbreaks and before vaccination, bDMARDs did not increase the risk of infection and death due to the SARS-CoV-2 virus in rheumatic patients.
On the other hand, MTX can increase, and hydroxychloroquine can decrease the risk of COVID-19 infection in rheumatic patients. There was no difference in the frequency of COVID-19 infection according to the type of rheumatic disease.
After the complete vaccination, further research is required to evaluate the correlation between rheumatic diseases, drugs, and new variants of the SARS-CoV-2 virus and determine the impact on the ability to produce antibodies against the virus and response to vaccinations.