
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune condition characterized by periods of exacerbation and remission [1–6]. A period of remission gives the patient hope of health improvement, while the period of disease exacerbation with all associated physical limitations results in depressed mood, depressive states and decreased life satisfaction.
Day by day, the patient experiences pain, his activity is restricted, he is dependent on other individuals and unable to exercise self-care [7, 8]. The sense of safety is uncertain, as it now depends on the patient’s care-givers and the rate of disease progression.
In the period of disease exacerbation, the patient experiences fear of the unknown and fear of his inability to affect the development of his situation. The patient comes under the rules established by the health care institutions and care-givers and it is on them that his future fate depends [9, 10]. Accepting the disease seems to be a tremendous problem for the patient [11].
Attention is very frequently paid to the patient’s adjustment to restrictions imposed by the disease. Accepting the condition may be difficult for the affected individual. Emotional disorders that are then seen in the patients may be contingent upon emotional burden, unknown course of disease progression and difficulties in daily life [12–16].
Often, the patients give up their social life, being afraid of their lack of resourcefulness due to the deformed joints, limited physical activity and constant pain. Due to their weakness and malaise they often stay at home unwilling to meet other people.
Avoiding social contacts results in disturbed emotional bonds with their family members and friends, which leads to their depressed mood because of constant solitude. The self-esteem of the patients is deteriorated, their willingness to fight for maintaining their dexterity subsides and in consequence such individuals become depressive or demonstrate other emotional disturbances [12, 17–22].
All the above factors significantly affect the acceptance of illness [23]. Rheumatoid arthritis is a condition that cannot be completely cured. Thus, in the case of RA, acceptance will involve getting to know the weak points of the disease, as well as the resources of the patient’s body and using the said knowledge to better cope with difficulties. Self-efficacy, acceptance of the illness and satisfaction with life undoubtedly contribute to preventing emotional disturbances and improving social functioning in patients with RA [12].
Material and methods
Study design
The objective of the study was to present social functioning of RA patients taking into consideration their age and employing selected determinants, i.e. satisfaction with life, generalized sense of self-efficacy and acceptance of illness.
The study was carried out using the diagnostic poll method and the questionnaire technique. Standardized tools were employed, i.e. the Satisfaction with Life Scale (SWLS), Generalized Self Efficacy Scale (GSES) and Acceptance of Illness Scale (AIS).
The Satisfaction with Life Scale includes five statements that may refer to the present life of the responder. The subject evaluates the degree to which the statements describe her/his life and the degree of her/his agreeing with such statements [24].
The Generalized Self Efficacy Scale is a tool composed of 10 questions that probe into the strength of the subject’s conviction regarding her/his successful coping with difficult and new situations [25].
The Acceptance of Illness Scale includes 8 statements describing the consequences of poor health. The consequences represent limitations imposed by the disease, such as lack of self-sufficiency, the sense of being dependent on other people and a decreased sense of self-esteem [26].
Inclusion criteria
The inclusion criteria for the study group were as follows: diagnosed rheumatoid arthritis; no concomitant inflammatory diseases of the musculoskeletal system; meeting the age criterion; no mental diseases, neurological diseases or other disability-causing high-grade conditions apart from RA; granting written informed consent to participate in the study.
The inclusion criteria for the control group: good health; no diseases of the musculoskeletal system; meeting the age criterion; no mental diseases, neurological diseases and other disability-causing high-grade conditions; granting written informed consent to participate in the study.
The study finally included 250 subjects (patients with RA and healthy non-RA subjects). The patients were assigned to disease exacerbation and disease remission groups. Information allowing a patient to be assigned to a given group was obtained from the staff members upon obtaining the consent of the patients and management of the institution. The patients with exacerbated disease and those belonging to the control group were subdivided into younger and older subjects. No such subdivision was employed in the patients in remission due to the small number of subjects.
Study population
The study group included patients with RA (males and females) in two age groups: 18–45 years (the younger group) and over 60 years (the older group). The control group consisted of non-RA subjects (males and females) belonging to two age groups: 18–45 years (the younger group) and over 60 years (the older group).
Statistical analysis
The analysis of quantitative variables was presented using the mean value, standard deviation value, median value, quartile value, minimum and maximum values. The qualitative variables were presented as the number and percentage value of each variable.
The analysis of the relationship between the qualitative variables was performed using the chi-square test (as corrected by Yates for 2 × 2 tables) or Fisher’s exact test (low anticipated values). The comparison of the values of the quantitative variables in the two groups was based on the Student’s t-test or the Mann-Whitney U test.
The comparison of the value of the quantitative variables in three or more groups was performed using analysis of variance (ANOVA). If statistically significant differences were found, post-hoc analysis was performed using Tukey’s HSD test or the Dunn test. The correlation between two quantitative variables was analyzed using Pearson’s or Spearman’s coefficients. The adopted significance level was α = 0.05.
In view of the low number of responders in the RA remission group, no analysis of comparison of the younger and older groups was performed.
Ethical standards
The ethical principles for medical research involving human subjects were respected in the presented study according to the Declaration of Helsinki. All patients gave their informed consent to the procedures described. A positive opinion was granted by the Bioethics Commission (KBET/166/B/2014).
Study groups
Characterization of rheumatoid arthritis patients in the exacerbation period
The group of RA patients with exacerbated disease numbered 100 individuals (the younger group – 46%: 18–45 years of age; x = 36, SD = 6.78; the older group – 54%: x = 71, SD = 7.21). The majority of the subjects had completed secondary education (41%). The remaining individuals were primary (8%), vocational (27%) or university school graduates (23%).
Disability certificates were held by 48% of the individuals, including 26% of moderate degree and 12% of severe degree certificates. Some of these patients used self-paid rehabilitation services (63%). A total of 16% of the study subjects in this group took advantage of self-paid visits in private rheumatology doctor’s offices.
On average, the patients traveled to such rheumatology offices 5 times per year. The mean distance between their home and the office was 42 kilometers, with the travel time of more than 1 hour (Table I).
Table I
Characterization of rheumatoid arthritis patients in the exacerbation period
| Property | Younger group (n = 46) | Older group (n = 54) | Total (n = 100) | p-value* | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex | 0.902 | ||||||
| Female | 38 | 82.6 | 43 | 79.6 | 81 | 81.0 | |
| Male | 8 | 17.4 | 11 | 20.4 | 19 | 19.0 | |
| Education | 0.01 | ||||||
| Primary | 2 | 4.4 | 6 | 11.1 | 8 | 8.0 | |
| Vocational | 8 | 17.4 | 19 | 35.2 | 27 | 27.0 | |
| Secondary | 19 | 41.3 | 22 | 40.7 | 41 | 41.0 | |
| University | 17 | 37.0 | 6 | 11.1 | 23 | 23.0 | |
| No data available | 0 | 0.0 | 1 | 1.9 | 1 | 1.0 | |
| Professional activity | |||||||
| Employed full-time | 21 | 46.0 | 3 | 5.6 | 24 | 24.0 | < 0.001 |
| Employed part-time | 5 | 10.9 | 0 | 0.00 | 5 | 5.0 | |
| Unemployed | 1 | 2.2 | 1 | 1.9 | 2 | 2.0 | |
| Old age pensioner/pensioner | 16 | 34.8 | 49 | 90.7 | 65 | 65.0 | |
| Student | 2 | 4.4 | 0 | 0.0 | 2 | 2.0 | |
| Self-employed | 1 | 2.2 | 1 | 1.9 | 2 | 2.0 | |
| Place of residence | |||||||
| Rural area | 24 | 52.2 | 31 | 57.4 | 55 | 55.0 | 0.492 |
| Medium-large town | 8 | 17.4 | 12 | 22.2 | 20 | 20.0 | |
| City | 14 | 30.4 | 11 | 20.4 | 25 | 25.0 | |
| Doctor’s office | |||||||
| State-financed | 32 | 69.6 | 52 | 96.3 | 84 | 84.0 | 0.001 |
| Private | 2 | 4.4 | 1 | 1.9 | 3 | 3.0 | |
| Some visits in a private office | 12 | 26.1 | 1 | 1.9 | 13 | 13.0 | |
| Disability certificate | |||||||
| Yes | 14 | 30.4 | 34 | 63.0 | 48 | 48.0 | 0.002 |
| No | 32 | 69.6 | 20 | 37.0 | 52 | 52.0 | |
| Degree of disability | |||||||
| Considerable | 1 | 2.2 | 11 | 20.4 | 12 | 12.0 | 0.003 |
| Moderate | 10 | 21.7 | 16 | 29.6 | 26 | 26.0 | |
| Mild | 3 | 6.5 | 7 | 13.0 | 10 | 10.0 | |
| None | 32 | 69.6 | 20 | 37.0 | 52 | 52.0 | |
| Self-financed rehabilitation services | |||||||
| Yes | 33 | 71.7 | 30 | 55.6 | 63 | 63.0 | 0.144 |
| No | 13 | 28.3 | 24 | 44.4 | 37 | 37.0 | |
| Property | Mean value (SD) | Median value (quartile value) | Mean value (SD) | Median value (quartile value) | Mean value (SD) | Median value (quartile value) | p-value** |
| Age | 36.61 (6.78) | 39 (33.25–41) | 70.76 (7.21) | 68 (66–76) | 55.05 (18.48) | 61.5 (39.75–69) | < 0.001 |
| Time of travel to see a rheumatologist [min] | 66.15 (45.54) | 60 (30–90) | 67.67 (48.37) | 60 (30–90) | 66.97 (46.86) | 60 (30–90) | 0.997 |
| Distance to the rheumatologist’s office [km] | 35.32 (31.74) | 25 ( 12.25–43.75) | 46.06 (41.26) | 30 (18–80) | 41.12 (37.39) | 27.5 (15–61) | 0.203 |
| Annual number of visits in the rheumatologist’s office | 5.2 (3.61) | 4 (3–6) | 4.57 (2.88) | 4 (3–4) | 4.86 (3.23) | 4 (3–5.25) | 0.934 |
The comparison of the study groups of the younger and older RA patients in the period of disease exacerbation showed differences. The younger group subjects were better educated, showed a higher professional activity, more often decided to visit private doctor’s offices, less frequently held disability certificates and demonstrated a lower degree of disability (p < 0.05) (Table I).
Characterization of rheumatoid arthritis patients in the remission period
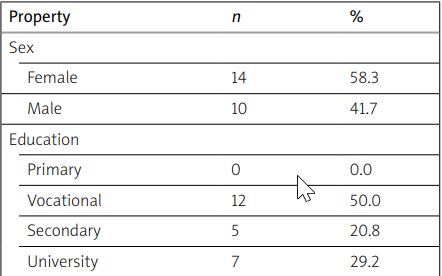
The group included 24 individuals (x = 51 years of age, SD = 16.38). The majority of these individuals had completed vocational (50%) and university (29%) education. The group included mainly old age pensioners and pensioners (54%). The majority of the subjects lived in large cities (> 100,000 inhabitants) (58%). Twenty-five percent of them had disability certificates (Table II).
Table II
Characterization of rheumatoid arthritis patients in the remission period
A significant percentage of the subjects used self-financed rehabilitation sessions (79%). The patients travelled to offices of rheumatology specialists 4 times a year on average. The mean distance between their homes and such offices was approximately 20 kilometers and their travel time was almost 45 minutes.
Characterization of the control group
The control group included 126 individuals. Younger subjects (18–45 years of age) accounted for 52% of the group members (x = 27 years of age). The majority of them completed secondary (26%) or university education (71%), were employed full-time (72%) and lived in large cities (> 100,000 inhabitants) (72%). Older individuals (> 60 years of age) accounted for 48% of all the subjects (x = 67 years of age); the majority of them were secondary school graduates (34) (61%).
Differences were found between the investigated groups, old-age pensioners or pensioners (79%). They mostly lived in large cities (> 100,000 inhabitants the younger and older subjects. The younger individuals were better educated, showed a higher degree of professional activity and somewhat more frequently lived in large cities (p < 0.05).
Results
Satisfaction with life
The sense of satisfaction with life in the RA patients in the exacerbation period was the most frequently described as low (55%) and less commonly as moderate (31%). The variable of satisfaction with life showed no statistically significant differences between the groups of the younger and older subjects (p > 0.05).
The sense of satisfaction with life in this group of patients was determined by their sex and education level (p < 0.05). The females were more extreme in their evaluation as compared to the males: the female subjects more frequently described their satisfaction with life as low, but they also often described it as high. The predominant description of satisfaction with life in the males was “moderate” (Table III).
Table III
Satisfaction with life in rheumatoid arthritis patients during the exacerbation period – comparison of age groups
| Satisfaction with life (SWLS) | Younger group | Older group | Total | p-value* | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Low | 24 | 52.2 | 31 | 57.4 | 55 | 55.0 | 0.660 |
| Moderate | 14 | 30.4 | 17 | 31.5 | 31 | 31.0 | |
| High | 8 | 17.4 | 6 | 11.1 | 14 | 14.0 | |
On the other hand, the younger vs. older female and male responders did not significantly differ with respect to their sense of satisfaction with life (p > 0.05). The subjects who had completed university education showed a higher sense of satisfaction with life as compared to the remaining individuals (p < 0.05). The group of the vocational school graduates included the highest number of the subjects describing their satisfaction with life as low (81%). The university-educated individuals were most often characterized as having a moderate (39%) or high (30%) sense of satisfaction with life (p < 0.05).
Both in the younger and older group of RA patients, satisfaction with life was significantly dependent upon education (p < 0.05). In the younger group, the highest satisfaction with life was reported by the university-educated responders and the lowest – by the individuals who had completed secondary education. A similar situation was noted in the older group.
In the group of 24 RA patients in remission, 54% of the subjects reported a moderate sense of satisfaction with life, 25% – high, and 20% of the patients reported low satisfaction with life.
In the control group, satisfaction with life was the most frequently described as high (41%) and moderate (39%). The younger and older subjects did not significantly differ in their satisfaction with life (p > 0.05).
Self-efficacy
The RA patients in the period of disease exacerbation were basically characterized by a low sense of self-efficacy (38%). Nevertheless, the number of the individuals reporting a high sense of self-efficacy was only slightly lower (35%). The reason here was the fact of considerable differences between the younger and older groups with respect to self-efficacy (p < 0.05). The sense of self-efficacy was higher in the group of younger individuals.
Of 24 responders to the questionnaire, 75% reported high, 17% low and 8% – moderate self-efficacy. In the control group, 60% of the subjects were characterized as having a high sense of self-efficacy. A considerably lower number reported a moderate (34%) and low (6%) sense of self-efficacy. The younger and older groups did not significantly differ in their sense of self-efficacy (p > 0.05).
A relationship was found between the answers obtained using the questionnaire of generalized sense of self-efficacy (GSES) in the RA patients during the exacerbation period and their education. The sense of self-efficacy was significantly dependent on education (p < 0.05). The highest self-efficacy was reported by the responders who had completed secondary education, while the lowest values were characteristic of the individuals with primary and vocational schooling. Similar percentages of the university-educated responders reported low, moderate and high generalized self-efficacy.
The highest number of primary school graduates reported low self-efficacy (57%), while the remaining subjects described self-efficacy as high (29%) and moderate (14%). In the group of the patients with secondary education, 39% reported high, 37% moderate and 24% low self-efficacy. Among the university-educated subjects, a similar number reported low (35%) and high (35%) self-efficacy, while 30% of the subjects reported moderate self-efficacy (Table IV).
Table IV
Generalized sense of self-efficacy in rheumatoid arthritis patients during the exacerbation period – comparison of age groups
| Self-efficacy (GSES) | Younger group | Older group | Total | p-value* | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Low | 10 | 21.7 | 28 | 51.8 | 38 | 38.0 | 0.004 |
| Moderate | 18 | 39.1 | 9 | 16.7 | 27 | 27.0 | |
| High | 18 | 39.1 | 17 | 31.5 | 35 | 35.0 | |
In the younger group, self-efficacy was not significantly related to education (p > 0.05). On the other hand, in the group of older patients, self-efficacy was significantly determined by the education level. The highest self-efficacy was reported by the secondary school graduates, while the individuals who had completed primary and vocational education showed the lowest self-efficacy (p < 0.05).
Acceptance of the illness
The mean value of acceptance of the illness by the RA patients during the period of disease exacerbation was 20.4. The groups of the younger and older patients significantly differed in their level of illness acceptance. The younger patients were more accepting of their illness as compared to the group of older RA patients (Table V).
Table V
Generalized sense of self-efficacy in rheumatoid arthritis patients during the exacerbation period – comparison of between the age groups
| Group | Acceptation of the Illness Scale [score] | p-value* | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | X | SD | Me | Min | Max | Q1 | Q3 | ||
| Younger group | 46 | 23.87 | 8.38 | 24.00 | 8.00 | 40.00 | 16.25 | 30.00 | < 0.001 |
| Older group | 54 | 17.44 | 6.48 | 19.00 | 8.00 | 35.00 | 11.00 | 22.75 | |
| Total | 100 | 20.40 | 8.05 | 21.00 | 8.00 | 40.00 | 13.75 | 25.25 | |
The mean score of acceptance of the illness in the patients in remission was 29.38 points. The level of acceptance of the illness was significantly related to the education level of the patients (p < 0.05). The accuracy of the relationship was tested using the post-hoc analysis.
As the analysis showed, the university-educated subjects were more accepting of their illness as compared to the individuals who had completed primary or vocational education. The younger group did not reveal any dependence between acceptance of the illness and education of the responders (p > 0.05). On the other hand, such a dependence was demonstrated in the group of older patients (p < 0.05).
The exactitude of the correlation was evaluated by the post-hoc analysis; as the assessment showed, the university-educated patients were more prone to accept their illness as compared to the subjects who had completed primary and vocational schools. Acceptance of the illness was not investigated among the comparison group subjects.
Correlations between questionnaires among rheumatoid arthritis patients with disease exacerbation
Among the young RA patients, statistical significance was observed in correlations between each questionnaire and the remaining consecutive questionnaires. The correlations were positive, which indicated that the higher the value in one questionnaire was, the higher was the score in another questionnaire. It followed that satisfaction with life, social support, generalized sense of self-efficacy and acceptance of the illness were directly related. The strongest correlation was seen between AIS and SWLS (p < 0.05) (Table VI).
Table VI
Correlation between satisfaction with life, self-efficacy and acceptance of the illness in rheumatoid arthritis patients during the exacerbation period
| Variables | Correlation coefficient | p-value | Direction of correlation | Correlation power | |
|---|---|---|---|---|---|
| SWLS | GSES | 0.468 | < 0.001 | Positive | Low |
| SWLS | AIS | 0.583 | < 0.001 | Positive | Moderate |
| GSES | AIS | 0.549 | < 0.001 | Positive | Moderate |
Discussion
Rheumatoid arthritis is a disease characterized by progressive joint destruction and later by extraarticular organic lesions. The RA considerably affects the patient’s social functioning, which is determined among other factors by as satisfaction with life, generalized sense of self-efficacy or acceptance of the illness [27–29].
A thorough review of literature addressing satisfaction with life and describing more than 66,000 responders demonstrated that the degree of their satisfaction with life was not dependent on their sex, but their age and cultural background were important for their evaluation score [30].
As it follows from the present study, in the RA patients in the period of disease exacerbation education significantly affected their satisfaction with life. The university-educated patients demonstrated high satisfaction with life; moreover, the female and male individuals in the group differed significantly in their sense of such satisfaction. The females were more extreme in their assessment as compared to the males: the former more commonly described their satisfaction with life as low, but also more commonly as high. Other studies evaluated satisfaction with life in the elderly [31].
One hundred two individuals with the mean age of 69 years of life were investigated. As many as 75% of the responders reported suffering from a chronic disease. The authors emphasized a moderate level of satisfaction with life in these subjects. Interestingly, high satisfaction with life on the borderline with moderate satisfaction level was observed in the males, while in the females, the responses showed a somewhat lower satisfaction level and moderate satisfaction scores were on the borderline with high level. Thus, it was not surprising that a high level of satisfaction with life was reported by the responders aged 75–89 years of life with secondary and university education [31].
In the present study, the sense of satisfaction with life in the healthy members of the comparison group was high, while the RA patients in the period of disease exacerbation showed in this field significant differences between the females and males. Similarly as in the above quoted report, the scores reported by the females demonstrated a pronounced contribution of emotions in defining satisfaction with life; the females more frequently described their satisfaction with life as low, yet they equally often rated it as high.
In the group of control individuals, the males and females did not significantly differ in their perceived satisfaction with life. On the other hand, in the group of younger responders, the female and male subjects significantly differed in their sense of satisfaction with life: the rating in the males was more diverse (a higher number of both low and high scores as compared to the females). In the group of older respondents, however, the females and males did not significantly differ in their sense of satisfaction with life.
Zalewska-Puchała et al. [32] evaluated satisfaction with life in 109 students of the Cracow University of the Third Age. Almost 25% of the students did not suffer from any disease and felt good, while 65% of the responders had chronic diseases. Almost 25% of the subjects reported a low level of satisfaction with life, 42% reported a moderate level and 33% were characterized by a high level of satisfaction [32].
On the other hand, the present study did not find any statistically significant differences between the younger and older group with respect to satisfaction with life. This was true for both the RA patients in the period of disease exacerbation and individuals from the control group.
Self-efficacy is believing that one is capable of meeting defined objectives and of controlling one’s activities. Expectations one has may determine undertaking specific behaviors. Such expectations are of a special importance in patients suffering from chronic diseases who throughout the duration of the illness must be firmly convinced on an ongoing basis they will be up to tasks they face in the therapeutic process. A high level of generalized self-efficacy may decrease anxiety, fear and difficulties which do not help in pursuing one’s objectives, as well as increase the belief in meaningfulness of one’s activities [26, 33].
Multi-center studies were carried out in north-east China in 305 RA patients. The investigation aimed among other things at demonstrating a relationship between generalized level of self-efficacy and fatigue in RA subjects. The GSES scale was employed. The mean level of generalized self-efficacy for all the patients was estimated as 18.27 – in keeping with the key of the scale, the number of points was within sten score 2, denoting a low level of self-efficacy in the Chinese population of RA patients.
Generalized sense of self-efficacy was significantly negatively correlated with fatigue, which meant the higher level of generalized self-efficacy being associated with a lower fatigue level [34]. The high level of self-efficacy in young subjects may contribute to better therapeutic success in the course of treatment [35].
As demonstrated in the present study, the young RA patients (18–45 years of age) in the exacerbation period assessed the level of self-efficacy as moderate and high. To use a comparison, in the healthy (control) responders the most numerous group of the young subjects indicated a high level of self-efficacy.
In the group of patients during the exacerbation period, the younger subjects were characterized by a higher sense of self-efficacy as compared to the older individuals, while in the group of healthy responders, the score for self-efficacy did not differ between the two age groups. Generalized self-efficacy in the older patients was significantly dependent on their age.
Jachimowicz and Kostka [36] carried out studies on self-efficacy among the elderly. The investigation included 104 residents of a nursing home. The investigators found a high sense of self-efficacy [36]. On the other hand, in the present study, a low sense of self-efficacy predominated in the group of older patients. In the above-mentioned report [36], the responders characterized by a high level of self-efficacy demonstrated its correlation with the highest level of satisfaction with life. Such a correlation was also demonstrated in the present study.
On the other hand, the higher the level of acceptance of illness in the patients, the better the level of adaptation to the situation imposed by the illness and the lower sense of disease-accompanying discomfort. The RA acceptance among patients was investigated by Szafraniec et al. [37]. The study included 40 RA subjects – both inpatients and outpatients staying in their home environment. The acceptance index was 26.45 points, which indicates a moderate acceptance level.
The investigators analyzed the group taking into consideration sex, education and age. The males were characterized by a considerably higher level of acceptance of illness as compared to the females. The females showed poorer adaptation to limitations imposed by RA. The responders with university education manifested the highest index of acceptance of illness, while the lowest index was observed among the primary school graduates.
While analyzing the results achieved by the responders with respect to their age, the investigators noted that the highest indices of acceptance of illness were characteristic for the young patients (up to 39 years of age), while the elderly (above 60 years of age) showed the lowest level of adaptation [37].
As found in the present study, the patients in remission more easily accepted their illness. Among the patients with exacerbated disease, the younger group (18–45 years of age) tended to accept their illness more readily as compared to the elderly (above 60 years of age). Also the female and male subjects did not significantly differ in their level of acceptance of their illness.
On the other hand, similarly as in case of the studies previously referred to, the level of disease acceptance depended on education. The university graduates were more willing to accept their illness as compared to the primary and vocational schools graduates. As found in other investigations performed in patients with chronic diseases, including individuals with locomotor system conditions, acceptance of their state of health was rated as 26.63 points [38].
The afore-mentioned studies, as well as the present investigation describe the mean score of illness acceptance within the range of 20–27 points, with 40 points as the maximum score to be obtained. This observation proves an insufficient level of acceptance of the illness in the responders, which may affect the overall functioning of such patients.
Rheumatic diseases, including RA constitute a serious social and economic problem. The highest costs result from disability seen in RA patients, which is associated with poor mental and social functioning [39, 40]. For this reason it is extremely important to preserve the ability of the patients to exercise self-care and accept their illness; thus reducing the economic, social and family-related costs associated with their suffering from RA [41, 42].
Conclusions
The RA patients in the period of disease exacerbation predominantly demonstrated low and moderate levels of satisfaction with life, in the patients in remission period the score was moderate, while the control group subjects defined their level of satisfaction with life as high and moderate.
The level of acceptance of illness was described by the RA patients in the period of disease exacerbation as insufficient. The patients in remission defined their level of acceptance of illness as better.
The patients with RA exacerbation generally showed a low sense of self-efficacy, yet a large group of such patients presented also high self-efficacy levels and the majority of the RA subjects in remission declared a high sense of self-efficacy.
In the RA patients, satisfaction with life, generalized sense of self-efficacy and acceptance of illness were closely related and affected general their psychosocial functioning.