
Introduction
Rheumatoid arthritis (RA), one of the most common systemic autoimmune diseases, is characterized by chronic and progressive systemic inflammation. It is mainly manifested as symmetrical peripheral polyarthritis; however, it may also be accompanied by several extra-articular manifestations and systemic comorbidities [1, 2]. Several studies have reported an increase in cognitive decline in RA patients, with prevalence ranging from 29 to 72.4% [3–7]. Cognitive impairment ranges from mild cognitive impairment (MCI) to dementia. Unfortunately, even mild cognitive decline can significantly reduce physical function in daily activities, quality of life, adherence to treatment, and self-care of RA patients [5, 8, 9].
The exact mechanism underlying cognitive impairment in RA remains unclear. A number of hypotheses have been proposed, including chronic inflammation affecting the blood–brain barrier and systemic inflammation accelerating atherosclerosis [8, 10, 11]. Additionally, cognitive functions may be affected by pain and depression in RA patients. Pain can affect memory and attention, while depression may cause problems with concentration and executive functions [12, 13]. Moreover, the effects of drugs commonly used in RA treatment, such as methotrexate (MTX) and glucocorticosteroids (GCs), have also been associated with cognitive impairment in RA [13–15]. It has also been suggested that the increased risk of cardiovascular diseases in RA patients could be involved in cognitive decline via mechanisms associated with metabolic syndrome and inflammatory proteins [5, 8]. During the last few years, a growing number of studies have investigated the predictive factors associated with cognitive impairment in RA patients, but the findings are inconsistent [6, 7, 10, 13].
Neuropsychological testing is useful for patients with suspected cognitive impairment, but its use is limited in daily practice due to its high cost and time-consuming nature. Therefore, a simple, feasible, valid, and reliable cognitive screening test is required in clinical practice. The Montreal Cognitive Assessment (MoCA) is a brief cognitive screening tool comprising 30 scorable items that can be completed in 10–15 minutes. The MoCA has been shown to be sensitive (90%) and specific (87%) for detecting mild cognitive impairment [16, 17]. It has been translated into Indonesian (MoCA-INA) and shown to have good validity and reliability [18].
There is currently a lack of research on the prevalence of cognitive impairment in Indonesian RA patients. Moreover, there is considerable variability in prevalence and clinical features among different ethnic groups [5, 19–21]. The objective of this study was to explore the prevalence and possible predictors of cognitive impairment in a cohort of RA individuals.
Material and methods
Study design and data collection
This cross-sectional study was conducted at Dr. Cipto Mangunkusumo National Referral Hospital. Patients visiting the Rheumatology Clinic were consecutively recruited from 2021 to 2023. The inclusion criteria of this study were patients aged ≥ 18 years with a well-established diagnosis of RA according to 2010 American College of Rheumatology/European League Against Rheumatism (EULAR) criteria, who were able to read and write, understood the Indonesian language, and agreed to be involved in this study. Rheumatoid arthritis patients with overlap syndrome or other autoimmune diseases, severe visual impairment, history of any significant neuropsychiatric illness (such as vascular dementia, neurodegenerative disorder, head trauma, cerebral infection, and cerebrovascular accident), psychosis or recent antipsychotics use within the preceding 6 months, or severe depression were excluded from this study.
Baseline demographic data, including personal history, duration of RA, comorbidities, and RA therapy, were collected. Physical examinations, including blood pressure measurement and tender and swollen joint examination, were performed by trained physicians on admission. Laboratory data on erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were obtained from medical records.
Disease activity was measured by Disease Activity Score in 28 joints, based on the ESR level (DAS28-ESR) and Disease Activity Score in 28 joints, based on the CRP level (DAS28-CRP). Data related to DAS28-ESR and DAS28-CRP included patient global assessment of health (0–10 cm Visual Analogue Scale), tender joint count (28 joints), swollen joint count (28 joints), ESR, and CRP. Cumulative disease activity of DAS28 was calculated by the sum of serial measurements of DAS28 divided by the total number of clinic visits from the first to last measurements.
Depression status was assessed using the Indonesian version of the Hospital Anxiety-Depression Scale (HADS) questionnaire. Depression was defined by a score of 8 or above [22]. Cognitive function was assessed using the MoCA-INA questionnaire, which was administered by trained physicians. The subjects were classified as cognitively impaired if they scored less than 26.
Statistical analyses
Data were analyzed using SPSS 25.0. Descriptive statistics were used to describe the basic characteristics and clinical variables of the sample. Categorical data were presented as percentages, while continuous data were presented as mean ± standard deviation or median (range). Bivariate analyses with the χ2 test, or Fisher’s test as an alternative, were performed to assess whether there was a significant difference between RA patients with or without cognitive impairment for the categorical variables. For comparison of continuous variables, the unpaired t-test (parametric test) or Mann-Whitney test (non-parametric test) was performed. A backward stepwise multivariate logistic regression analysis was conducted on the independent variables with a p-value < 0.25 on bivariate analysis, in order to identify the predictive factors of cognitive impairment in RA patients. A p-value < 0.05 was considered statistically significant.
Results
Characteristics of subjects
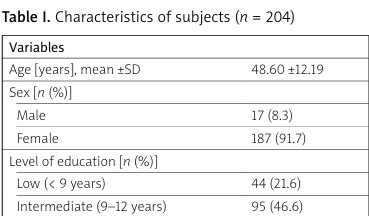
A total of 204 participants were included in the analysis, with a mean age of 48.60 ±12.19 years. The majority were female (91.7%) and had an intermediate level of education (46.6%). Most of the subjects used MTX (79.9%), either as monotherapy or in combination with other disease-modifying antirheumatic drugs (DMARDs), and 66.2% used GC. According to HADS scores, 5.9% of participants had depression and 14.7% had anxiety. Characteristics of the subjects are further detailed in Table I.
Table I
Characteristics of subjects (n = 204)
[i] BMI – body mass index, CRP – C-reactive protein, csDMARDs – conventional synthetic disease-modifying antirheumatic drugs, DAS28 – Disease Activity Score in 28 joints, DMARDs – disease-modifying antirheumatic drugs, ESR – erythrocyte sedimentation rate, GCs – glucocorticosteroids, HADS – Hospital Anxiety-Depression Scale, MoCA-INA – Montreal Cognitive Assessment-Indonesian, MTX – methotrexate, SD – standard deviation.
The prevalence of cognitive impairment based on the MoCA-INA score in this study was 54.9%, with an overall median MoCA-INA score of 25 (range: 3–30). Subjects in the cognitively impaired group scored significantly lower in nearly all the MoCA domains: visuospatial/executive, naming, attention, delayed recall, abstraction, and language. Scores of each MoCA-INA cognitive domain among RA patients with and without cognitive impairment are presented in Table II.
Table II
Scores of each cognitive domain based on MoCA-INA in RA patients with or without cognitive impairment
| Cognitive domain of MoCA-INA | Total* (n = 204) | Impaired cognitive function* (n = 112) | Normal cognitive function* (n = 92) | p |
|---|---|---|---|---|
| Total score | 25 (3–30) | 23 (3–25) | 27 (26–30) | < 0.001† |
| Visuospatial/executive | 4 (0–5) | 3.5 (0–5) | 4 (2–5) | < 0.001† |
| Naming | 3 (0–3) | 3 (0–3) | 3 (2–3) | 0.003† |
| Attention | 5.5 (0–8) | 5 (0–6) | 6 (3–8) | < 0.001† |
| Language | 2 (0–3) | 2 (0–3) | 3 (1–3) | < 0.001† |
| Abstraction | 2 (0–2) | 1 (0–2) | 2 (1–2) | < 0.001† |
| Delayed recall | 3 (0–5) | 2 (0–5) | 4 (0–5) | < 0.001† |
| Orientation | 6 (0–6) | 6 (0–6) | 6 (5–6) | 0.058† |
Analysis of factors associated with cognitive impairment
Table III presents the results of bivariate analysis comparing various demographic, clinical, and laboratory characteristics between the normal and cognitively impaired groups. The cognitively impaired group was significantly older (MD = 5.56, 95% CI: 2.26–8.86, p = 0.001) and had a higher proportion of individuals with low and intermediate education level compared to the normal cognitive group (p = 0.002 and p = 0.026, respectively).
Table III
Comparison between cognitively normal and impaired
| Variables | Impaired cognitive (n = 112) | Normal cognitive (n = 92) | p | OR (95%) or MD (95%) |
|---|---|---|---|---|
| Sex [n (%)] | ||||
| Male | 9 (52.9) | 8 (47.1) | 0.865a | 0.92 (0.34–2.48) |
| Female | 103 (55.1) | 84 (44.9) | ||
| Age [years], mean ±SD | 51.11 ±11.31 | 45.54 ±12.57 | 0.001b | 5.56 (2.26–8.86) |
| Education [n (%)] | ||||
| Low | 31 (70.5) | 13 (29.5) | 0.002a | 3.58 (1.58–8.09) |
| Intermediate | 55 (57.9) | 40 (42.1) | 0.026a | 2.06 (1.09–3.92) |
| High | 26 (40.0) | 39 (60.0) | Ref | |
| Duration of disease [years], median (min–max) BMI, median (min–max) | 2.00 (0.08–19.00) | 2.00 (0.08–34.00) | 0.758c | – |
| 23.36 (15.06–43.18) | 22.92 (13.62–36.11) | 0.830c | – | |
| Hypertension [n (%)] | ||||
| Yes | 24 (51.1) | 23 (48.9) | 0.547a | 0.82 (0.43–1.57) |
| No | 88 (56.1) | 69 (43.9) | ||
| Diabetes mellitus [n (%)] | ||||
| Yes | 18 (69.2) | 8 (30.8) | 0.116a | 2.01 (0.83–4.86) |
| No | 94 (52.8) | 84 (47.2) | ||
| Obesity [n (%)] | ||||
| Yes | 30 (50.0) | 30 (50.0) | 0.364a | 0.76 (0.41–1.38) |
| No | 82 (56.9) | 62 (43.1) | ||
| Smoking [n (%)] | ||||
| Yes | 2 (40.0) | 3 (60.0) | 0.498a | 0.54 (0.09–3.30) |
| No | 110 (55.3) | 89 (44.7) | ||
| GCs use [n (%)] | ||||
| Yes | 80 (59.3) | 55 (40.7) | 0.080a | 1.68 (0.94–3.02) |
| No | 32 (46.4) | 37 (53.6) | ||
| Methotrexate use [n (%)] | ||||
| Yes | 91 (55.8) | 72 (44.2) | 0.596a | 1.20 (0.61–2.39) |
| No | 21 (51.2) | 20 (48.8) | ||
| ESR [mm/h], median (min–max) | 36 (1–131) | 37 (1–115) | 0.864c | – |
| CRP [mg/l], median (min–max) | 2.75 (0.10–106.00) | 3.00 (0.10–90.30) | 0.908c | – |
| Cumulative DAS28-ESR, median (min–max) | 3.28 (0.80–6.15) | 3.43 (1.46–6.32) | 0.914c | – |
| Cumulative DAS28-CRP, median (min–max) | 2.42 (0.96–7.10) | 2.45 (0.96–5.20) | 0.729c | – |
| Depression [n (%)] | ||||
| Yes | 8 (66.7) | 4 (33.3) | 0.399a | 1.69 (0.49–5.81) |
| No | 104 (54.2) | 88 (45.8) | ||
| Anxiety [n (%)] | ||||
| Yes | 17 (56.7) | 13 (43.3) | 0.833a | 1.09 (0.50–2.38) |
| No | 95 (54.6) | 79 (45.4) | ||
BMI – body mass index, CRP – C-reactive protein, DAS28 – Disease Activity Score in 28 joints, DAS28-CRP – Disease Activity Score in 28 joints, based on the CRP level, DAS28-ESR – Disease Activity Score in 28 joints, based on the ESR level, ESR – erythrocyte sedimentation rate, GCs – glucocorticosteroids, MD – mean difference, OR – odds ratio, SD – standard deviation.
Variables with a p-value < 0.25 in bivariate analysis were further included in the multivariate analysis. Age, education level, diabetes mellitus, and GC use were included in the multivariate logistic regression model. The results showed that older age (OR = 1.045, 95% CI: 1.018–1.073, p = 0.001), low education level (OR = 2.260, 95% CI: 1.153–4.432, p = 0.018), intermediate education level (OR = 3.161, 95% CI: 1.359–7.353, p = 0.008), and GC use (OR = 2.147, 95% CI: 1.133–4.070, p = 0.019) were significant independent predictors of cognitive impairment in this study (Table IV).
Discussion
In this study, we investigated the prevalence and factors associated with cognitive impairment among a cohort of RA patients, as assessed by the MoCA-INA questionnaire. Our main results indicated that older age, lower education levels, and GC use were significant predictors of cognitive impairment in this population.
More than half of our RA subjects were cognitively impaired, with a prevalence of 54.9%. Impairments were identified in visuospatial/executive, naming, attention, delayed recall, abstraction, and language domains. There was variability regarding the prevalence of cognitive impairment in RA patients and the main cognitive domains impaired across different studies. For instance, Appenzeller et al. [4] reported a 30% prevalence of cognitive impairment using the Mini-Mental State Examination among RA patients in Brazil, compared to 7.5% in healthy controls, with notable deficits in verbal fluency, short-term memory, and logical memory. In another study from Thailand, Katchamart et al. [7] reported a 70% prevalence of cognitive impairment based on MoCA-Thai, with impairments in visuospatial/executive, language, and abstraction domains. This variability could be attributed to differences in the methods or tools used to assess cognitive dysfunction and sociodemographic factors.
Our findings align with previous evidence highlighting an increased prevalence of cognitive impairment among RA patients. Although the mechanisms linking RA and cognitive decline remain incompletely understood, neuroimaging studies might provide some insight. Bartolini et al. [3], for example, observed hypoperfusion in the frontal-parietal lobes on brain single-photon-emission computed tomography, possibly resulting from microangiopathy which disrupts the cortical-subcortical connection. Consequently, this may contribute to the findings of defective visuo-spatial and planning functions and impaired attention in their RA patients [3]. Furthermore, the impairment in attention suggests the possible role of chronic pain in interfering with maintenance of memory traces when performing complex tasks, thus causing disruptions in attentional processes [23, 24]. Chronic inflammation in RA patients may damage the endothelium in the blood-brain barrier, allowing autoantibodies and inflammatory mediators to diffuse into the brain parenchyma, thereby causing neuroinflammation and demyelination and ultimately leading to cognitive impairment [8].
Older age and lower education levels were demographic factors associated with cognitive impairment in both individuals with RA and the general population. Age is a known risk factor of cognitive impairment; however, the presence of RA may significantly contribute to its faster decline. Several studies have shown that cognitive decline begins to occur after the age of 60 years [25]. However, it is noteworthy that the mean age of RA patients with cognitive impairment in this study (51.11 ±11.31 years) was considerably younger than the non-RA population. This is supported by the findings of a study by Mo et al. [26], which demonstrated accelerated cognitive decline in RA patients compared to controls. Aside from chronic inflammation, age may affect cognitive function in RA patients through the increase of senescent CD8+CD28– T-cells, which is negatively correlated with memory function, as well as increased comorbidities and cardiovascular risk in elderly RA patients, which can lead to cerebral hypoperfusion and neurodegeneration [8]. Therefore, interventions designed to prevent age-related cognitive decline in RA patients should be initiated earlier and may include physical activity (particularly resistance training), cognitive training, and the management of vascular risk factors such as hypertension, obesity, and smoking [27, 28].
Individuals with a lower educational level were at an increased risk of cognitive impairment in our study, consistent with previous findings [29, 30]. It is hypothesized that higher education is linked to a greater cognitive reserve, through enhancement of synaptic density and neural plasticity, thus related to slower neurodegenerative changes and cognitive decline [30]. Our findings are particularly relevant given that low educational level has also been associated with worse outcomes in RA, including disease severity and functional status [31, 32]. Furthermore, limited education may also serve as a barrier to patient health education, which is important in RA disease management and treatment adherence [33, 34].
Use of GC was another predictor of cognitive impairment in our study. This result is consistent with findings from previous studies [5]. Although GCs are important in RA treatment, particularly as bridging therapy before DMARD efficacy is achieved, their receptors are located in brain regions critical for cognition, such as the hippocampus, amygdala, and frontal lobes, raising concerns about their impact on memory and executive function [8, 14]. Excessive circulatory levels of GCs have been associated with cognitive impairment in various diseases [35]. Furthermore, a meta-analysis revealed that GC had a negative effect on executive function and memory, even in acute and short-term use [36]. This also supports the current 2022 EULAR recommendations, which emphasizes the rapid tapering and eventual discontinuation of GCs in RA management [37].
Several RA-related factors, such as disease activity and inflammatory markers, have been reported to be associated with cognitive impairment in previous research [7, 38, 39]. However, these were not identified as significant predictors in our study. This discrepancy may be due to sample size limitations or the cross-sectional design, which does not capture longitudinal fluctuations in disease activity and their cognitive impacts over time. Similarly, although depression has been reported to be negatively associated with cognition in RA and to mediate the pain-cognition relationship, it did not emerge as a significant predictor in our analysis [40]. This may be attributed to the relatively low prevalence of depression (5.9%) in our sample and different screening method of depression used.
Study limitations
This study has several limitations. First, as a cross-sectional study, it is not possible to assess the temporal relationship between cognitive impairment and RA. In addition, the baseline cognitive function prior to the onset of RA was also not assessed. Second, the absence of an age-matched healthy control group limits the ability to compare cognitive performance between RA patients and the general population.
Finally, this study did not analyze other factors that potentially affect cognitive function in RA patients, such as inflammatory mediators and autoantibodies, which may play important roles in cognitive dysfunction in RA.
Conclusions
In this study, cognitive impairment was identified in 54.9% of RA patients, with deficits observed across multiple domains, including visuospatial/executive function, naming, attention, delayed recall, abstraction, and language. Older age, lower educational level, and GC use emerged as significant predictors of cognitive impairment. Routine cognitive screening is recommended for all RA patients, particularly those at higher risk, to enable early detection and treatment when cognitive decline is found.