
Introduction
Systemic lupus erythematosus (SLE) is a multifaceted autoimmune disease driven by dysregulation of the immune system, particularly through the abnormal activation of T and B lymphocytes [1]. That leads to the production of autoantibodies and immune complexes that trigger inflammation, resulting in tissue and organ damage. The disease predominantly affects women of childbearing age [2]. Despite advancements in treatment, mortality rates in SLE remain notably high, particularly among older patients, with infections and cardiovascular complications being the primary causes of death [3, 4]. Thus, SLE diagnosed in patients older than 50 (late-onset SLE – Lo-SLE) presents distinct clinical challenges, including diagnostic delays, a higher multimorbidity burden, and the need for tailored therapeutic strategies to minimize long-term complications associated with ageing [5].
The pathogenesis of Lo-SLE, including sex hormone levels, differs from that of early-onset SLE (Eo-SLE, diagnosed before age 50) [4, 6, 7]. Late-onset SLE represents about 2–20% of all SLE cases, with a lower female-to-male ratio than Eo-SLE [4, 7]. Patients with Lo-SLE typically experience a more insidious disease progression, encounter the classic symptoms less frequently, and exhibit lower disease activity than Eo-SLE [8]. Autoantibody profiles also differ regarding the age of SLE onset [4]. For example, Lo-SLE exhibits lower frequencies of anti-double-stranded DNA (dsDNA), anti-nucleosome, anti-Smith (Sm), and anti-ribonucleoprotein (RNP) antibodies compared to Eo-SLE [7]. Inversely, rheumatoid factor is found more frequently in Lo-SLE [4]. Moreover, older patients often had medical comorbidities, and their initial SLE signs and symptoms could be misinterpreted. Consequently, the disease onset might not be diagnosed promptly [4, 9]. The course of Lo-SLE presents with less organ involvement, but certain manifestations such as arthritis, pleuritis, pericarditis, myositis, pulmonary fibrosis, and associated Sjögren’s disease (SjD) have been reported more frequently [4, 7]. Additionally, Lo-SLE patients may have a higher incidence of thromboembolism with positive laboratory test results for antiphospholipid syndrome (APS) [7]. However, findings on these manifestations remain inconsistent across studies [4, 9]. In some of them, organ damage appears to be more prevalent in the Lo-SLE group, which could be related to iatrogenic factors such as osteoporosis and age-related health issues. Therefore, the question arises about the perception of Lo-SLE as a milder SLE form [7].
In the Polish population, there is still a lack of comprehensive studies exploring clinical and laboratory differences between Lo-SLE and Eo-SLE patients [9]. Therefore, we decided to analyze the clinical and laboratory characteristics of Lo-SLE in a large cohort of SLE patients treated at our hospital and compare them to those of Eo-SLE. By identifying distinct patterns and potential risk factors, we seek to contribute to improved personalized management for SLE patients across different age groups.
Material and methods
Study population
A retrospective analysis was conducted using medical records of adult patients diagnosed with SLE (using disease code ICD10: M32) at the University Hospital in Krakow, Poland, from 2012 to 2022. All included patients fulfilled the classification criteria established by the 2019 European Alliance of Associations for Rheumatology (EULAR) and American College of Rheumatology (ACR) guidelines [10].
Our previous publication described the methods in detail [11]. Data collection included comprehensive demographic information (e.g., age, sex, and family history of autoimmune diseases), clinical manifestations, and laboratory findings. Specific data points included the timing of symptom onset and diagnosis, disease duration, systemic comorbidities, miscarriage history (for female patients), therapeutic interventions, and, where applicable, the cause and age at death. “Age at diagnosis” was defined as the age at the time of SLE diagnosis by a physician, according to the SLE classification criteria. “Age at symptoms” was defined as the age at which the first symptoms related to lupus occurred. Clinical manifestations assessed encompassed skin involvement, joint symptoms, serositis, hematological abnormalities, organ-specific conditions (affecting kidneys, liver, nervous system, or respiratory system), Raynaud’s phenomenon (RP), and lymphadenopathy. Neuropsychiatric lupus was assessed using the 1999 ACR criteria [12]. For detailed definitions, see our previous publication [11].
Patients were then divided into 2 groups based on their age at the time of diagnosis: those with Lo-SLE, defined as diagnosis at or after the age of 50, and those with Eo-SLE, diagnosed before the age of 50.
Laboratory analysis
Laboratory assessments were performed using standard methods, including complete blood cell count analyses, lipid profile, creatinine level (with glomerular filtration rate estimated by the MDRD formula), 24-hour urine protein excretion, and urine sediment evaluation. Antinuclear antibodies (ANA) were detected using indirect immunofluorescence on HEp-2 cell slides. Further identification of specific antibodies was conducted using enzyme-linked immunosorbent assay (ELISA) or line-blot immunoassay, including the evaluation of anti-dsDNA antibody presence. Anti-dsDNA antibodies were additionally assessed on slides using Crithidia luciliae as the substrate to increase the specificity and sensitivity of the analyzed methods. Serum complement levels were measured by nephelometry. Tests for antiphospholipid antibodies (aPLA) included assessments of lupus anticoagulant, anti-cardiolipin antibodies, and anti-b2-glycoprotein I antibodies (both IgM and IgG classes). Laboratory tests were performed at a third-grade reference laboratory by a diagnostic analyst specializing in immunology.
Statistics analysis
Data analysis was conducted using STATISTICA Tibco 13.3 software (StatSoft Inc., Tulsa, OK, USA). Categorical variables were presented as frequencies and percentages. Comparisons between groups were performed using either the χ2 test or Fisher’s exact test, as appropriate. The Shapiro-Wilk test was employed to assess normality, indicating that all continuous variables were non-normally distributed. Consequently, these variables were reported as medians with Q1–Q3 ranges and analyzed using the Mann-Whitney test. Odds ratios (ORs) with 95% confidence intervals (95% CI) were calculated based on receiver operating characteristic curve analysis. Statistical significance was defined as a p-value of less than 0.05.
Results
Demographic features
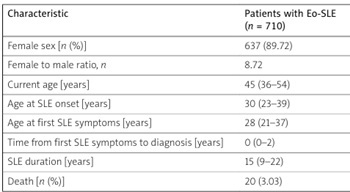
A summary of the demographic characteristics is provided in Table I. Early-onset SLE and Lo-SLE patients were similar in terms of sex, with a high predominance of females in both groups. As expected, the Lo-SLE patients were older, with older age at SLE onset and first symptoms, but with shorter SLE duration. Interestingly, a higher mortality rate was also documented in these patients (OR = 4.10, 95% CI: 2.02–8.33, p < 0.001). Table II presents detailed information on the causes of death among patients with SLE.
Table I
Demographic characteristics of patients with early-onset and late-onset systemic lupus erythematosus
Table II
Detailed characteristics of death causes in patients with early-onset and late-onset systemic lupus erythematosus
Lower frequency of central nervous system and kidney involvement and higher prevalence of interstitial lung disease in late-onset systemic lupus erythematosus patients
Table III summarizes the cumulative frequencies of systemic symptoms across the SLE study groups. Overall, in the Eo-SLE group, the most prevalent clinical manifestations included hematological (90.85%) and joint (88.87%) symptoms, as well as mucocutaneous manifestations (82.68%). On the other hand, the Lo-SLE group exhibited comparable predominant symptoms, with hematological (81.59%), joint (80.60%), and constitutional (74.63%) signs being the most frequent.
Table III
Cumulative frequencies of systemic involvement in patients with early-onset and late-onset systemic lupus erythematosus
| Clinical manifestations | Patients with Eo-SLE (n = 710) | Patients with Lo-SLE (n = 201) | p |
|---|---|---|---|
| Constitutional symptoms [n (%)] | 540 (76.06) | 150 (74.63) | 0.68 |
| Fever | 307 (44.62) | 57 (28.64) | < 0.001 |
| Fatigue/weakness | 433 (62.94) | 118 (59.6) | 0.39 |
| Myalgias | 266 (38.66) | 70 (35.35) | 0.40 |
| Weight loss | 141 (20.55) | 45 (22.61) | 0.53 |
| Lymphadenopathy | 139 (20.17) | 19 (9.6) | < 0.001 |
| Mucocutaneus manifestations [n (%)] | 587 (82.68) | 142 (70.65) | < 0.001 |
| Lupus malar rash | 317 (45.22) | 72 (36) | 0.020 |
| Discoid rash | 63 (8.99) | 13 (6.5) | 0.26 |
| Urticaria | 63 (8.99) | 7 (3.5) | 0.01 |
| Cutaneous vasculitis | 45 (6.42) | 9 (4.5) | 0.31 |
| Alopecia | 200 (28.45) | 28 (14) | < 0.001 |
| Oral and/or nasal ulcers | 115 (16.41) | 22 (11) | 0.06 |
| Photosensitivity | 233 (33.24) | 69 (34.33) | 0.77 |
| Other skin changesa | 474 (67.33) | 115 (57.5) | 0.010 |
| Joint manifestations [n (%)] | 631 (88.87) | 162 (80.6) | 0.002 |
| Arthritis | 438 (62.48) | 91 (45.27) | < 0.001 |
| Arthralgia | 627 (88.81) | 163 (81.1) | 0.004 |
| Serositis [n (%)] | 166 (23.85) | 42 (21) | 0.40 |
| Pleural effusion | 112 (15.84) | 35 (17.41) | 0.59 |
| Pericardial effusion | 99 (14.22) | 23 (11.5) | 0.32 |
| Pericarditis | 30 (4.25) | 4 (2) | 0.14 |
| Hematological manifestations [n (%)] | 645 (90.85) | 164 (81.59) | < 0.001 |
| Leucopeniab | 446 (64.64) | 89 (45.64) | < 0.001 |
| Lymphopeniac | 499 (74.15) | 128 (67.37) | 0.06 |
| Anemiad | 486 (70.23) | 124 (63.27) | 0.06 |
| Hemolytic anemiae | 61 (19.61) | 18 (16.51) | 0.48 |
| Thrombocytopeniaf | 220 (31.93) | 56 (28.57) | 0.37 |
| Macrophage activation syndrome | 7 (1) | 1 (0.51) | 0.51 |
| Thrombotic thrombocytopenic purpura | 2 (0.28) | 0 (0) | 0.45 |
| Kidney involvement [n (%)] | 294 (41.41) | 49 (24.38) | < 0.001 |
| 24-hour urinary protein excretion > 0.5 g/day | 249 (36.19) | 37 (18.97) | < 0.001 |
| 24-hour urinary protein excretion > 3.5 g/day | 126 (19.27) | 17 (8.95) | < 0.001 |
| Urinary casts | 106 (17.29) | 12 (6.42) | < 0.001 |
| Erythrocyturia | 182 (28.04) | 34 (17.71) | 0.004 |
| Leucocyturia | 212 (32.02) | 37 (19.07) | < 0.001 |
| Neurological signs [n (%)] | 72 (10.21) | 14 (7) | 0.17 |
| Central nervous system involvement | 51 (7.23) | 5 (2.5) | 0.014 |
| Peripheral nervous system involvement | 33 (4.68) | 9 (4.5) | 0.91 |
| Raynaud’s phenomenon [n (%)] | 192 (27.16) | 27 (13.43) | < 0.001 |
| Lung involvement [n (%)] | 45 (6.48) | 27 (13.5) | 0.001 |
| Interstitial lung disease | 27 (3.84) | 19 (9.45) | 0.001 |
| Diffuse alveolar hemorrhage | 6 (0.85) | 3 (1.49) | 0.42 |
| Pulmonary hypertension | 18 (2.59) | 8 (4) | 0.30 |
| Lupoid hepatitis [n (%)] | 34 (4.81) | 13 (6.47) | 0.35 |
However, compared to the Eo-SLE group, the Lo-SLE cohort less frequently exhibited systemic clinical manifestations, including fever (OR = 0.50, 95% CI: 0.35–0.71, p < 0.001) and lymphadenopathy (OR = 0.42, 95% CI: 0.24–0.71, p < 0.001). In the Lo-SLE group, mucocutaneous manifestations were also less frequent, such as lupus malar rash (OR = 0.68, 95% CI: 0.49–0.95, p = 0.023), urticaria (OR = 0.37, 95% CI: 0.14–0.82, p = 0.010), RP (OR = 0.42, 95% CI: 0.26–0.65, p < 0.001), and alopecia (OR = 0.41, 95% CI: 0.26–0.64, p < 0.001). Likewise, arthritis and arthralgias were less common in these patients (OR = 0.50, 95% CI: 0.36–0.69, p < 0.001 and OR = 0.54, 95% CI: 0.35–0.85, p = 0.006, respectively), similar to all hematological manifestations, e.g., leucopenia (OR = 0.46, 95% CI: 0.33–0.64, p < 0.001).
Additionally, the Lo-SLE group in comparison to Eo-SLE was characterized by less frequent kidney involvement, defined by the presence of urinary casts (OR = 0.33, 95% CI: 0.16–0.62, p < 0.001), 24-hour urinary protein excretion > 0.5 g/day (OR = 0.41, 95% CI: 0.27–0.62, p < 0.001), 24-hour urinary protein excretion > 3.5 g/day (OR = 0.41, 95% CI: 0.23–0.71, p < 0.001), leucocyturia (OR = 0.50, 95% CI: 0.33–0.75, p < 0.001), and erythrocyturia (OR = 0.55, 95% CI: 0.36–0.84, p = 0.004). Table IV presents the results of kidney biopsies in SLE patients with lupus nephritis, classified according to the International Society of Nephrology/Renal Pathology Society criteria.
Table IV
Summary of lupus nephritis classes according to the International Society of Nephrology/Renal Pathology Society (ISN/RPS) criteria in early-onset and late-onset systemic lupus erythematosus patients with lupus nephritis
On the other hand, the only more frequent Lo-SLE clinical manifestation was interstitial lung disease (OR = 2.61, 95% CI: 1.34–5.00, p = 0.003). Finally, patients with Lo-SLE exhibited a lower incidence of central nervous system involvement (OR = 0.33, 95% CI: 0.10–0.84, p = 0.012).
Higher frequency of medical comorbidities in patients with late-onset systemic lupus erythematosus
As expected, the Lo-SLE patients more frequently suffered from medical comorbidities than Eo-SLE patients (Table V). In the former group, particularly common were those predisposing or related to cardiovascular events, such as arterial hypertension (OR = 3.49, 95% CI: 2.44–5.05, p < 0.001), diabetes mellitus (OR = 2.67, 95% CI: 1.63–4.32, p < 0.001), hypercholesterolemia (OR = 1.52, 95% CI: 1.09–2.10, p = 0.010), atrial fibrillation (OR = 3.55, 95% CI: 1.68–7.45, p < 0.001), peripheral artery obliterans disease (OR = 3.33, 95% CI: 1.72–6.40, p < 0.001), myocardial infarction (OR = 3.59, 95% CI: 1.94–6.6, p < 0.001), and heart failure (OR = 2.65, 95% CI: 1.36–5.07, p = 0.003).
Table V
Cumulative frequencies of comorbidities in patients with early-onset and late-onset systemic lupus erythematosus
| Characteristic | Patients with Eo-SLE (n = 710) | Patients with Lo-SLE (n = 201) | p |
|---|---|---|---|
| Hypothyroidism [n (%)] | 169 (23.87) | 50 (24.88) | 0.77 |
| Hyperthyroidism [n (%)] | 35 (4.94) | 8 (3.98) | 0.57 |
| Arterial hypertension [n (%)] | 320 (45.07) | 149 (74.13) | < 0.001 |
| Diabetes mellitus [n (%)] | 52 (7.32) | 35 (17.41) | < 0.001 |
| Heart failurea [n (%)] | 27 (3.81) | 19 (9.5) | 0.001 |
| Hypercholesterolemiab [n (%)] | 311 (43.87) | 109 (54.23) | 0.009 |
| Atrial fibrillation [n (%)] | 18 (2.54) | 17 (8.46) | < 0.001 |
| Peripheral artery obliterans disease [n (%)] | 24 (3.38) | 21 (10.45) | < 0.001 |
| End-stage kidney disease [n (%)] | 20 (2.83) | 5 (2.49) | 0.80 |
| MGUS [n (%)] | 5 (0.7) | 10 (4.98) | < 0.001 |
| Malignancy [n (%)] | 54 (7.61) | 37 (18.59) | < 0.001 |
| Arterial thrombotic episode [n (%)] | 59 (8.32) | 42 (20.9) | < 0.001 |
| Stroke | 48 (6.76) | 21 (10.45) | 0.08 |
| Transient ischemic attack | 10 (1.41) | 4 (2) | 0.55 |
| Myocardial infarct | 27 (3.8) | 25 (12.44) | < 0.001 |
| Other arterial thrombotic episodes | 14 (1.97) | 6 (2.99) | 0.39 |
| Venous thrombotic episode [n (%)] | 122 (17.26) | 37 (18.41) | 0.70 |
| Deep venous thrombosis | 107 (15.09) | 29 (14.43) | 0.82 |
| Pulmonary embolism | 26 (3.67) | 11 (5.47) | 0.25 |
| Deep venous thrombosis and pulmonary embolism | 16 (2.26) | 5 (2.49) | 0.85 |
| Other venous thrombotic episodes | 9 (1.27) | 6 (2.99) | 0.09 |
| Miscarriage | 85 (16.04) | 17 (12.69) | 0.34 |
Categorical variables are presented as numbers with percentages, and continuous variables are presented as medians with Q1–Q3 ranges.
a Symptoms of heart failure, left ventricular ejection fraction of ≤ 40%, or diagnosis based on medical history.
In Lo-SLE patients, malignancy and monoclonal gammopathy of undetermined significance occurred more often (OR = 2.77, 95% CI: 1.71–4.45, p < 0.001, and OR = 7.36, 95% CI: 2.26–27.77, p < 0.001, respectively).
Distinct antibody profiles in patients with late-onset and early-onset systemic lupus erythematosus
All patients exhibited positive ANA results as determined by the indirect immunofluorescence (Table VI). In patients with Lo-SLE, we observed a lower prevalence of SLE-specific antibodies, including anti-dsDNA (OR = 0.62, 95% CI: 0.43–0.90, p = 0.009), anti-nucleosome (OR = 0.50, 95% CI: 0.33–0.75, p < 0.001), and anti-histone (OR = 0.48, 95% CI: 0.30–0.75, p < 0.001) antibodies. Regarding other autoantibodies, anti-SSB antibodies were more frequently detected (OR = 1.46, 95% CI: 1.01–2.09, p = 0.040), whereas anti-RNP antibodies were less prevalent (OR = 0.40, 95% CI: 0.23–0.67, p < 0.001). Concerning APS, lupus anticoagulant and anti-cardiolipin antibodies in the IgG class were less frequently present in Lo-SLE patients (OR = 0.51, 95% CI: 0.32–0.79, p = 0.002). Importantly, in the Eo-SLE group, thrombotic events were significantly more frequent among aPLA-positive patients compared to aPLA-negative individuals. Arterial thromboses occurred in 13.68% (n = 32/234) vs. 4.44% (n = 4/90), p = 0.010; venous thromboses in 27.20% (n = 96/353) vs. 12.03% (n = 19/158), p < 0.001; and any thrombosis in 35.13% (n = 124/353) vs. 17.09% (n = 27/158), p < 0.001. In the Lo-SLE group, rates of thrombotic events did not differ significantly between aPLA-positive and aPLA-negative patients: arterial thromboses in 26.32% (n = 10/38) vs. 15.00% (n = 3/20), p = 0.51; venous thromboses in 33.85% (n = 22/65) vs. 23.68% (n = 9/38), p = 0.27; and any thrombosis in 47.69% (n = 31/65) vs. 34.21% (n = 13/38), p = 0.18.
Table VI
Autoantibody profile in patients with early-onset and late-onset systemic lupus erythematosus
| Parameter (number of patients with analyzed parameter) | Patients with Eo-SLE (n = 710) | Patients with Lo-SLE (n = 201) | p |
|---|---|---|---|
| ANA – IIF assay, titera | 1 : 5,120 (1 : 2,560–1 : 20,480) | 1 : 5,120 (1 : 2,560–1 : 20,480) | 0.50 |
| Anti-SjDA antibodiesb [n (%)] | 397 (59.25) | 107 (58.79) | 0.91 |
| Anti-SjDB antibodiesb [n (%)] | 185 (27.61) | 65 (35.71) | 0.030 |
| Anti-histone antibodiesb [n (%)] | 189 (28.21) | 29 (15.93) | < 0.001 |
| Anti-nucleosome antibodiesb [n (%)] | 231 (34.48) | 38 (20.88) | < 0.001 |
| Anti-Smith antibodiesb [n (%)] | 82 (12.28) | 16 (8.84) | 0.20 |
| Anti-RNP antibodiesb [n (%)] | 158 (23.62) | 20 (11.05) | < 0.001 |
| Anti-dsDNA antibodiesb [n (%)] | 250 (37.37) | 59 (32.96) | 0.28 |
| Anti-dsDNA antibodiesc [n (%)] | 443 (69.76) | 99 (58.93) | 0.008 |
| Anti-dsDNA antibodies (positive in any of the analyzed methods) [n (%)] | 481 (74.69) | 115 (68.86) | 0.13 |
| Lupus anticoagulant [n (%)] | 158 (30.56) | 22 (20) | 0.030 |
| Anti-cardiolipin antibodies IgG and/or IgM [n (%)] | 319 (56.16) | 60 (48.78) | 0.14 |
| Anti-cardiolipin antibodies IgG | 243 (42.93) | 34 (27.64) | 0.002 |
| Anti-cardiolipin antibodies IgM | 217 (38.48) | 45 (36.59) | 0.70 |
| Anti-β2 glycoprotein I IgG and/or IgM [n (%)] | 112 (24.78) | 27 (28.72) | 0.42 |
| Anti-β2 glycoprotein I IgG | 77 (17.11) | 15 (16.13) | 0.82 |
| Anti-β2 glycoprotein I IgM | 74 (16.48) | 21 (22.34) | 0.17 |
Interestingly, among patients with Eo-SLE but not Lo-SLE, the presence of anti-RNP antibodies was significantly associated with higher frequency of constitutional symptoms (OR = 1.87, 95% CI: 1.16–3.01) including fever, fatigue/weakness; serositis (OR = 1.97, 95% CI: 1.32–2.93) such as pleural effusion, pericardial effusion and pericarditis; hematological manifestations (OR = 4.27, 95% CI: 1.52–12.00), including leucopenia, lymphopenia, hemolytic anemia, and thrombocytopenia; and RP (OR = 3.65, 95% CI: 2.50–5.33).
Patients with late-onset systemic lupus erythematosus were less frequently treated with immunosuppressive medications
Next, we analyzed the various approaches to immunosuppressive therapy (Table VII). Glucocorticosteroids (GCs) were the most commonly administered treatment for both the Eo-SLE and Lo-SLE groups. However, Lo-SLE received this medication slightly less frequently (95.19% and 91.46%, respectively, p = 0.040). Likewise, Lo-SLE patients were less frequently prescribed certain immunosuppressive regimens, including belimumab (OR = 0.19, 95% CI: 0.02–0.75, p = 0.008), azathioprine (OR = 0.31, 95% CI: 0.21–0.46, p < 0.001), cyclosporine (OR = 0.36, 95% CI: 0.14–0.80, p = 0.007), mycophenolate mofetil (OR = 0.44, 95% CI: 0.29–0.66, p < 0.001), cyclophosphamide (OR = 0.44, 95% CI: 0.28–0.66, p < 0.001), and chloroquine or hydroxychloroquine (OR = 0.45, 95% CI: 0.32–0.64, p < 0.001).
Table VII
Treatment patterns in patients with early-onset and late-onset systemic lupus erythematosus
Discussion
The present study reveals clinical and laboratory characteristics of a large cohort of SLE patients from a single center, focusing on those diagnosed before the age of 50 compared to those diagnosed at 50 years or older. Our findings revealed that the age of onset significantly impacts the clinical presentation and progression of the disease. These distinctions offer valuable insights into overall prognosis, including the likelihood of organ-related complications and mortality. Our study describes one of the largest Polish cohorts of SLE patients in the literature, comparing various aspects of the disease based on the age of SLE onset.
In general, most SLE patients had early-onset disease, consistent with the current literature on this topic [5]. Late-onset SLE is used in the literature when the disease is diagnosed after the age of 50–65 years, although most studies use 50 years as the threshold [5, 6]. Interestingly, in our cohort of Eo-SLE and Lo-SLE patients, we noted a high prevalence of the female sex in both groups but with a slightly lower female-to-male ratio in the Lo-SLE group. According to the literature, female-to-male ratios in Eo-SLE and Lo-SLE differ, with lower values in Lo-SLE patients [5]. Interestingly, a Spanish multicenter registry cohort (RELESSER group) reported an almost two-fold lower female-to-male ratio in the Lo-SLE group [6]. Likewise, a study on a Polish cohort noted that the prevalence of SLE in males was higher in Lo-SLE compared to younger patients [9]. On the other hand, Aljohaani et al. [8] found similar percentages, similar to our study, of females in late-onset and younger-onset SLE groups (84.9% vs. 86.4%), potentially due to differences in inclusion criteria for the younger-onset group. These distinctions in sex ratios in SLE highlight the potential role of different underlying factors, such as genetic and hormonal influences, in the age-related onset of the disease.
In both groups, hematological and joint symptoms were the most common, which is consistent with previous studies on large SLE cohorts [6, 13]. However, the Eo-SLE cohort exhibited a higher prevalence of a broader range of clinical manifestations, including general symptoms (fever, lymphadenopathy), hematological (leukopenia), skin manifestations (alopecia, urticaria, lupus malar rash), and kidney and central nervous system involvement. This observation aligns with a report published by Riveros Frutos et al. [6], who found that hematological, renal, neuropsychiatric, and skin changes were the most frequent in the Eo-SLE group. Also in line with those results are data presented by Bindroo et al. [14], with alopecia, RP, and lymphadenopathy reported more frequently in Eo-SLE than Lo-SLE. Next, a meta-analysis by Medlin et al. [15] demonstrated, in contrast to our results, that serositis and pleuritis can also be found more frequently in the Eo-SLE group. On the other hand, interstitial lung disease was more frequently observed in Lo-SLE in our data and also in other studies [14, 16]. These findings suggest the possibility of overlap syndromes, such as SLE/SjD, which may contribute to lung involvement in these patients [17]. The same association is further supported by the higher prevalence of anti-SSB antibodies, characteristic of SjD, in Lo-SLE, which was published in the literature [17] and also documented in our data. Furthermore, Catoggio et al. [16] found sicca symptoms more frequent in older SLE patients, which also suggests suspicion of SjD. Unfortunately, data on sicca symptoms or overlapping autoimmune diseases such as SjD were not available for our cohort.
In our data, neuropsychiatric SLE was also less frequent in Lo-SLE than in Eo-SLE patients. This observation is in line with previously published data by Pamuk et al. [18], where symptoms of neuropsychiatric SLE were 1.41-fold more common in younger patients. In contrast, Jeleniewicz et al. [9] did not find differences in the frequency of neuropsychiatric SLE symptoms regarding patient age, likely attributable to the limited sample size of the studied groups.
We also found that Lo-SLE was characterized by a higher prevalence of medical comorbidities and malignancies, which may be linked to the age-related nature of these conditions and has been reported previously by other authors [6, 19, 20]. Moreover, similarly to our findings, specific comorbidities, such as arterial hypertension or dyslipidemia, may also influence the outcome of SLE [6]. Interestingly and consistent with previous data, arterial thromboembolic episodes were observed more frequently in Lo-SLE, specifically myocardial infarction [21]. Additionally, in our stratified analysis, thrombotic events were significantly more frequent in aPLA-positive patients with Eo-SLE, supporting the interpretation of these events as clinical manifestations of APS. In contrast, in Lo-SLE, thromboses occurred at similar rates regardless of aPLA status (positive vs. negative), suggesting they may reflect comorbidities or age-related vascular risk rather than APS.
In our data, the Lo-SLE group was characterized by a lower frequency of positive results for lupus anticoagulant and anti-cardiolipin antibodies in the IgG class. Moreover, SLE-characteristic ANA types were more common in Eo-SLE. This observation largely agrees with data presented in the review by Piga et al. [7], who highlighted a lower prevalence of anti-dsDNA, anti-nucleosome, anti-Sm, anti-RNP antibodies, and lupus anticoagulant positivity in Lo-SLE. Furthermore, this serological profile could influence or reflect the disease course, including treatment mode [7]. We observed a similar high prevalence of anti-dsDNA antibodies in Eo-SLE and Lo-SLE groups as measured by the Crithidia luciliae assay or immunoblotting. However, when these antibodies were assessed by the Crithidia luciliae assay characterized by higher sensitivity and specificity [22], their prevalence in patients from the Eo-SLE group increased. In contrast to our findings, Padovan et al. [23] reported a higher prevalence of anti-dsDNA antibodies in Lo-SLE. However, similar to our results, anti-SSB, and in some cases, anti-SSA antibodies, were more frequently present in Lo-SLE [7]. Another interesting finding of our study concerns the association between anti-RNP antibodies and clinical signs of Eo-SLE but not Lo-SLE. In the former group only, the presence of anti-RNP antibodies was related to the higher frequency of constitutional symptoms, serositis, hematological abnormalities, and RP. This observation aligns with a report by Riveros Frutos et al. [6], in which anti-RNP antibodies were significantly more common in patients with Eo-SLE, particularly in those with systemic symptoms such as fever, hematologic manifestations, serositis, and RP. According to them, anti-RNP antibodies were less common in Lo-SLE patients and were not associated with any specific clinical features [6].
Regarding therapy mode, both subgroups were treated the most frequently with GCs, chloroquine, or hydroxychloroquine, which aligns with EULAR recommendations from 2019 [24]. Furthermore, considering that most Eo-SLE patients presented with more signs of the disease, including kidney involvement and neuropsychiatric manifestations, they required frequent immunosuppressive drugs [6]. Adverse effects of that aggressive treatment, such as the increased risk of infections and organ toxicity, necessitate careful use in older patients [25]. Likewise, drug interactions underscore the importance of individualized pharmacotherapy in optimizing safety and efficacy in Lo-SLE [26].
Finally, we observed a higher mortality rate in Lo-SLE compared to Eo-SLE, which mirrors other data on SLE [6, 27]. In the study by Riveros Frutos et al. [6], mortality was higher in the Lo-SLE group when compared to Eo-SLE patients (14.3% vs. 4.7%, p < 0.001). A study by Viveiros et al. [27] documented that very late-onset SLE patients (≥ 60 years at the time of diagnosis) had the lowest survival rate compared to younger SLE groups, including those with SLE diagnosis between 50 and 59 years.
Study limitations
The retrospective design of this study introduces potential biases in data collection and patient selection, which could affect the reliability of the findings. Additionally, the single-center nature of the study may restrict the applicability of the results to a broader population. Essential lifestyle factors, such as smoking, alcohol consumption, physical activity, and dietary habits, were not accounted for in the database. Furthermore, key laboratory and clinical data, including inflammatory markers, lupus disease activity indices, and sicca symptoms, were unavailable for this cohort. The higher clinical incidence of thrombosis in Lo-SLE, despite lower frequencies of antiphospholipid antibodies, suggests a potential non-immune-mediated etiology or low test sensitivity. Therefore, these results should be interpreted cautiously. Moreover, due to the retrospective nature of the study, the use of disease activity indices, such as SLEDAI, was not feasible. This limitation stemmed from the absence of specific data required for score calculation at potential control time points and the variability in patient follow-up duration. A further limitation of the study is the lack of analysis regarding the impact of specific treatments on disease outcomes. Finally, some observed associations may be coincidental and not indicate causal relationships.
Conclusions
Late-onset SLE patients exhibited distinct clinical characteristics compared to Eo-SLE, with fewer disease-related manifestations, suggesting that these individuals may require less intensive immunosuppressive therapy. Notably, interstitial lung disease was more prevalent among older patients, highlighting a need for closer monitoring of pulmonary complications in this group. Furthermore, Lo-SLE was associated with a higher burden of medical comorbidities, malignancies, and arterial thromboembolic events, emphasizing the importance of a comprehensive approach to managing these patients. The ANA profile in Lo-SLE also differed, showing a reduced variety and frequency of autoantibodies, apart from anti-SSB antibodies, which may indicate a greater likelihood of overlap with SjD. Our findings underscore the need for further research to validate this potential association and optimize care for Lo-SLE patients.