
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disorder that primarily affects joints, leading to pain, swelling, and eventual joint damage. Both genetic and environmental factors play a role in the onset and progression of the disease. The chronic inflammatory process in RA can also damage extra-articular organs, including the kidney, heart, lung, eye, digestive system, skin, and nervous system [1]. Synovial hyperemia is a hallmark of active RA and psoriatic arthritis (PsA). The expansion of the synovial lining in arthritis increases the vascular supply to the synovium, to cope with the increased requirement for oxygen and nutrients. Ultrasound (US) imaging is a common method used in the diagnosis of arthritis that is non-invasive, accessible, reproducible and – importantly – also inexpensive compared to e.g. magnetic resonance imaging.
Ultrasound is not included in the diagnostic criteria for RA, but it serves as a valuable adjunct to the physical examination and is highly sensitive in detecting effusion and synovial hypertrophy. In healthy joints, synovium is not visible in US examination, but ultrasonographic assessment of synovium is helpful especially in patients with early arthritis. Through the use of US, we can visualize even slight synovial hypertrophy, and application of Power Doppler ultrasonography (PDUS) may confirm synovial hypervascularity. Using high-frequency linear probes, sensitive Doppler, and harmonic imaging, US has the potential to reveal even slight synovial hypertrophy. Elevated serum levels of low-density lipoprotein cholesterol (LDL-C) and apolipoprotein B 100, the main structural protein of LDL, are directly associated with risk of atherosclerotic cardiovascular events [2]. Typically, systemic inflammation can alter serum lipid levels, often resulting in elevated LDL-C and total cholesterol (TC) despite reduced high-density lipoprotein cholesterol (HDL-C), and these changes may be related to the intensity of inflammatory vascularization of the synovial membrane. This single-center study aimed to evaluate whether serum LDL-C levels are associated with the degree of synovial vascularization, as assessed by quantitative PDUS, in active RA and PsA patients.
Material and methods
The study was conducted at the Department of Early Arthritis Clinic in the National Institute of Geriatrics, Rheumatology, and Rehabilitation in Warsaw, Poland. A total of 80 patients participated, including 60 with RA and 20 with PsA.
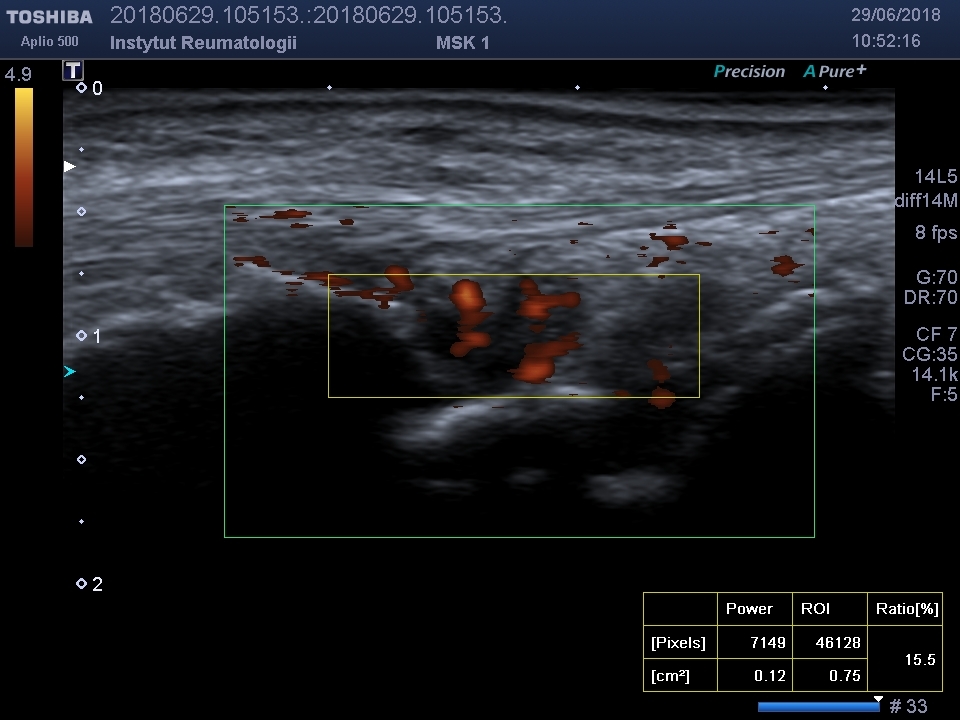
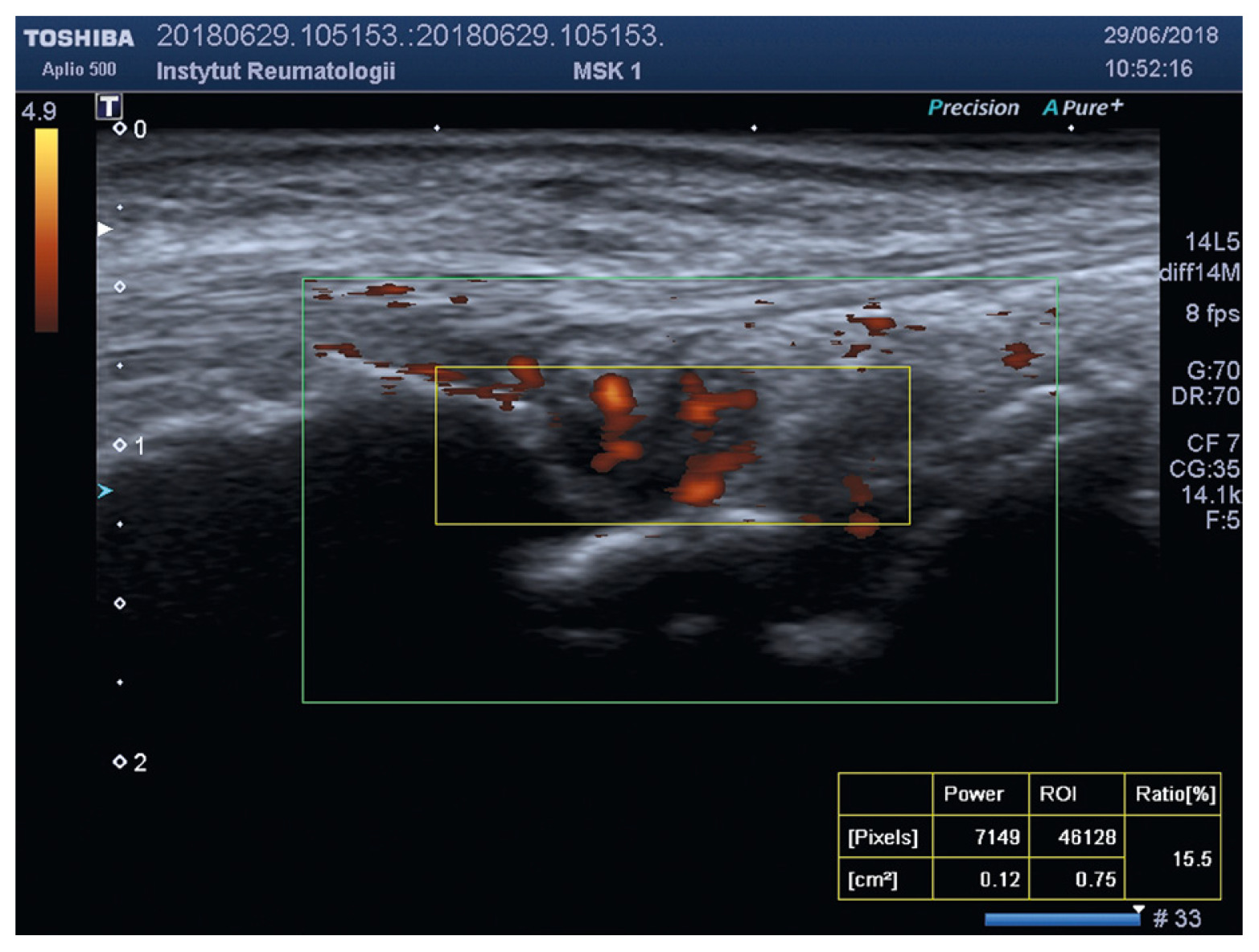
Diagnosis of RA was confirmed based on the 2010 American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology criteria, while PsA was diagnosed according to the ClASsification for Psoriatic ARthritis (CASPAR) criteria. Participants ranged in age from 26 to 81 years. The majority had been living with their condition for around two years, with an average disease duration of 8 years (SD ±8.41). The duration ranged from one month to 44 years, although 75% of the patients had been ill for less than 11 years. Characteristics of the whole study population are presented in Table I. Only individuals with high disease activity and peripheral articular involvement, with clinical presentation resembling RA (i.e., predominantly symmetric polyarthritis of small joints), were included. Psoriatic arthritis patients with predominant axial involvement or enthesitis were excluded. All joint assessments were conducted by the same rheumatologist with over a decade of clinical experience. Most of the participants were women (n = 53; 66.25%). Individuals with active infections, malignancies, recent injuries, other rheumatologic diseases, or conditions that could elevate inflammatory markers were excluded. The mean age of the study group was 54.65 years (SD ±14.23). Laboratory evaluations included rheumatoid factor (RF), anti-citrullinated protein antibodies (ACPA), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and LDL-C. Disease activity was measured using Disease Activity Score with 28 joints using the erythrocyte sedimentation rate (DAS28-ESR) and the Simplified Disease Activity Index (SDAI). All imaging was performed using the same US system (Toshiba Aplio 500) by a single radiology and imaging specialist. The study focused on evaluating the metacarpophalangeal joints, proximal interphalangeal joints, and wrists. Power Doppler US was used to assess joint vascularization, with vascular activity quantified via the PDUS index (INDEX%) within a defined region of interest (Fig. 1).
Table I
Characteristics of whole study population
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 27.0; IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated for all continuous variables and presented as means ± standard deviations (SD) or medians with interquartile ranges, as appropriate. Categorical variables were presented as frequencies and percentages (Table II). Normality of distribution was assessed using the Shapiro-Wilk test. Pearson correlation coefficients (r) were used to examine bivariate relationships between serum LDL-C levels and synovial vascularity (Power Doppler Index – INDEX%) when assumptions of normality were not met.
Table II
Descriptive statistics of variables
[i] CRP – C-reactive protein, DAS28 – Disease Activity Score in 28 joints, Dom – mode, ESR – erythrocyte sedimentation rate, INDEX% – percentage synovial vascularity score on power Doppler ultrasound, LDL – low-density lipoprotein cholesterol, M – mean, Max – maximum, Mdn – median, Min – minimum, SD – standard deviation, SDAI – Simplified Disease Activity Index.
To identify independent predictors of INDEX%, a multiple linear regression model was constructed. The dependent variable was INDEX%, and the independent variables included: disease group (RA vs. PsA, dichotomous), LDL-C (continuous), ACPA, RF, DAS28, and SDAI (Table III).
Table III
Correlations between variables
| Variable | ESR | CRP | DAS28 | SDAI | LDL |
|---|---|---|---|---|---|
| CRP | 0.61** | ||||
| DAS28 | 0.71** | 0.43** | |||
| SDAI | 0.61** | 0.97** | 0.56** | ||
| LDL-C | –0.10 | –0.06 | –0.19 | –0.15 | |
| INDEX% | 0.11 | 0.10 | 0.15 | 0.11 | –0.15 |
Interaction terms between disease group and LDL-C were explored to evaluate potential effect modification. Correlations between variables were performed at a significance level of 0.01 or 0.05. A p-value < 0.05 was considered statistically significant. Two multivariate linear regression models were constructed to evaluate predictors of synovial vascularity (INDEX%). Model 1 included demographic and inflammatory markers: age, ESR, CRP, LDL-C, and disease group (RA/PsA). Model 2 incorporated composite disease activity indices: age, DAS28, SDAI, LDL-C, and disease group. In both models, the intercept represents the expected INDEX% for the reference category. Adjusted standard errors (SE*) were applied. The objective was to compare how traditional inflammatory markers (model 1) vs. composite clinical scores (model 2) relate to synovial vascularity (Tables IV and V).
Table IV
Coefficients of predictors in model 1
| b | SE* | t | p | |
|---|---|---|---|---|
| Intercept | 22.131 | 8.016 | 2.761 | 0.007 |
| Age | 0.079 | 0.110 | 0.723 | 0.472 |
| ESR | 0.057 | 0.073 | 0.790 | 0.432 |
| CRP | 0.030 | 0.092 | 0.323 | 0.748 |
| LDL-C | –0.054 | 0.038 | –1.433 | 0.156 |
| Group | 1.292 | 3.296 | 0.392 | 0.696 |
Table V
Coefficients of predictors in model 2
| b | SE* | t | p | |
|---|---|---|---|---|
| Intercept | 6.717 | 13.331 | 0.504 | 0.616 |
| Age | 0.077 | 0.108 | 0.714 | 0.478 |
| DAS28 | 2.723 | 2.506 | 1.087 | 0.281 |
| SDAI | 0.018 | 0.084 | 0.211 | 0.833 |
| LDL-C | –0.047 | 0.039 | –1.199 | 0.234 |
| Group | 1.127 | 3.203 | 0.352 | 0.726 |
Results
Rheumatoid arthritis mean activity DAS28 was 6.11; PsA mean activity DAS28 was 5.9. All patients had active disease according to at least one of the applied disease activity scores, with DAS28 (ESR) ranging from 4.8 to 8.3 and SDAI from 23 to 183. In both groups, LDL-C serum level ranged from 31 to 194.2 mg/dl (mean 105.3); in 76.2%, LDL-C concentration was within the normal range; in 33.8%, serum LDL-C concentration was elevated. Mean LDL-C level in the RA group was 97.48 mg/dl, in the PsA group 113.17 mg/dl. There was no significant correlation between LDL-C serum concentration and INDEX% for both groups (r = 0.2). In model 1, only the intercept reached statistical significance (p = 0.007), while none of the individual predictors (age, ESR, CRP, LDL-C, group) showed significant associations with INDEX% (all p > 0.05). In model 2, likewise, none of the predictors (age, DAS28, SDAI, LDL-C group) were significantly associated with INDEX%. Low-density lipoprotein showed a negative trend in both models (model 1: β = –0.054, p = 0.156; model 2: β = –0.047, p = 0.234), though not statistically significant.
Overall, neither model yielded statistically significant predictors, suggesting that INDEX% may not be directly associated with routine systemic inflammatory markers or composite indices in this sample.
The results of the study were presented as part of a larger study during the ACR Congress in San Diego in 2023 in the form of a poster (Abstract ID ACR 2023: 1565472) [3].
Discussion
In both RA and PsA, chronic inflammation of the synovial membrane occurs due to the autoimmune process. The synovium undergoes excessive proliferation, becomes thickened, and is infiltrated by T lymphocytes, macrophages, and plasma cells. The migration of these inflammatory cells is facilitated by excessive angiogenesis, i.e., the formation of new blood vessels [4]. In PsA, as in RA, the synovial membrane proliferates, but the process is generally less aggressive. The inflammatory infiltrate is dominated by neutrophils, macrophages, and Th17 and Th1 lymphocytes, which play a key role in the pathogenesis of PsA [5].
Hypercholesterolemia has long been considered the most common risk factor for cardiovascular diseases. Low-density lipoproteins significantly affect the condition of blood vessels, particularly in terms of vascular damage and the development of atherosclerosis [6]. Low-density lipoprotein penetrates the vascular endothelium and accumulates in the intimal layer of arteries. Once oxidized (ox-LDL), it becomes even more atherogenic, triggering an inflammatory response. Macrophages engulf ox-LDL, transforming into foam cells – a key component of atherosclerotic plaque. Additionally, LDL-C contributes to endothelial dysfunction by reducing nitric oxide production, a critical factor for vasodilation. Low-density lipoprotein also activates inflammatory cells that release proinflammatory cytokines (e.g., tumor necrosis factor [TNF], interleukin [IL]-6). Chronic vascular inflammation and endothelial damage increase the adhesion of monocytes and platelets, accelerating atherosclerosis [7]. The accumulation of LDL-C and plaque formation contributes to vascular stiffness.
Considering the effect of LDL-C on vascular health, the present study examined the correlation between serum LDL-C levels and synovial membrane vascularization – a marker of active arthritis – in patients with RA and PsA. As the results show, LDL-C levels ranged from 31 to 194.2 mg/dl (mean: 105.3 mg/dl), with 76.2% of patients having LDL-C within the normal range, and 33.8% showing elevated LDL-C levels. However, no correlation was found between LDL-C concentration and increased synovial vascularization, as measured by the PDUS index (INDEX%), in either the RA or the PsA group. These findings are consistent with the lipid paradox – a phenomenon in which individuals with lower LDL-C or TC levels experience worse outcomes in certain diseases (e.g., heart failure, cancer, or infections), despite high TC generally being considered a cardiovascular risk factor [8]. Studies have shown that patients with chronic heart failure and ischemic heart disease with lower TC levels may have higher mortality compared to those with elevated cholesterol levels [9]. In older adults, low TC may also be associated with increased mortality, challenging the traditional view of cardiovascular prevention. This could be due to reverse causality, where low TC is a consequence rather than a cause of severe illness, as seen in advanced cancers and infections, which negatively impact survival. Cholesterol is also believed to have protective properties: it is essential for cell membrane structure and steroid hormone synthesis, and may exhibit anti-inflammatory effects [10]. Moreover, TC interacts with the immune system. Higher TC levels may offer protection against infections, as lipoproteins can bind bacterial and viral toxins – a relationship observed during the SARS-CoV-2 pandemic [11, 12]. This is not the first study to assess lipid levels in patients with RA and PsA. Yan et al. [13] described lipid profile changes in RA, noting that LDL-C and TC levels are often reduced in RA patients, especially during periods of high inflammation. This contrasts with the increased cardiovascular risk in RA and is known as the lipid paradox. Systemic inflammation and proinflammatory cytokines such as IL-6, IL-1, and TNF may alter HDL structure and subcomponents, reducing its antiatherogenic capacity, promoting LDL oxidation and atherosclerotic plaque formation. Dysfunctional HDL-C may further disrupt LDL-C metabolism, thereby increasing cardiovascular risk. However, the exact mechanisms behind lipid alterations and elevated cardiovascular disease risk in RA remain unclear.
Cholesterol levels clearly fluctuate during inflammatory joint diseases. A prospective study by Van Every et al. [14] showed that higher LDL-C levels measured close to RA diagnosis or at the end of follow-up were associated with a lower risk of developing RA.
In PsA, the situation may differ slightly. Patients with PsA are more commonly affected by metabolic risk factors, including atherosclerosis, hyperlipidemia, and insulin resistance – often attributed to chronic inflammation. Effective treatment of psoriasis or PsA can help reduce cardiovascular risk [15]. Although similar proinflammatory cytokines are involved in the pathogenesis of both PsA and RA (e.g., TNF), metabolic disturbances are more frequently observed in psoriasis patients [16]. Individuals with psoriasis or PsA often present with altered lipid profiles, including elevated TC, LDL-C, triglycerides, and lipoprotein(a) [Lp(a)], as well as decreased HDL-C. Additionally, these patients may have dysfunctional LDL and HDL particles, small dense LDL, impaired LDL efflux, or abnormalities in apolipoproteins and oxidized LDL. The severity of PsA may be linked to the concentration of small dense LDL particles [17].
To date, evidence of the lipid paradox in PsA remains limited. One earlier study by Akkara et al. [18] explored changes in lipid profiles before and after psoriasis onset, comparing psoriasis patients with a control group over a 10-year period (5 years before and 5 years after diagnosis). They found significant decreases in TC and LDL-C levels in both groups, though the reduction was more pronounced in the non-psoriasis cohort.
Study limitations
The limitation of the study was the different number of patients in the RA and PsA groups. Additionally, the study included patients with high disease activity; therefore, it was not analyzed how the concentration of LDL-C correlates with the synovial blood supply in the case of lower disease activity. The study did not include data on how many patients used cholesterol-lowering drugs.
A limitation of the present study is the smaller number of PsA patients compared to those with RA, which precluded a direct comparison between groups in terms of the lipid paradox. For this reason, all patients were analyzed as a single cohort. Future studies should include a larger PsA group to enable a more thorough comparison.
Conclusions
Synovial membrane vascularity, measured as INDEX%, was similarly high in RA and PsA groups, confirming active disease.
No correlation was found between serum LDL-C levels and INDEX%, suggesting that LDL-C levels do not significantly influence synovial membrane vascularization in patients with active RA and PsA.
The majority of patients in both groups (76.2%) had normal serum LDL-C levels, consistent with the lipid paradox in the context of systemic inflammation.