
Introduction
Rheumatology is a rapidly evolving medical specialty that focuses on autoimmune connective tissue diseases, inflammatory joint diseases, regional rheumatological conditions, and some overuse injuries. Most of these disorders are chronic and potentially require the use of long-term remedies. However, these conditions often require long-term follow-up and continuous multi-disciplinary care. Consequently, the various rheumatology associations the value of patients’ awareness of their diseases and the benefit of shared knowledge in selecting optimal strategies to control diseases and to improve or maintain their quality of life [1].
Patient education is a crucial aspect of managing patients with inflammatory arthritis, such as rheumatoid arthritis. The main goal of increasing patients’ knowledge about their diseases is to allow active collaboration between patients and healthcare providers to facilitate optimal disease management [2].
Public awareness of rheumatology is deficient, and knowledge about autoimmune disorders is inaccurately perceived in many countries. Moreover, “although rheumatology is a subspecialty of internal medicine,” many individuals cannot differentiate it from orthopedics, which is a surgical branch [3, 4].
Furthermore, many people with painful overuse and mechanical regional rheumatological conditions under-estimate their illness and do not seek advice until the condition becomes advanced and the pain threshold is exceeded [5].
Patients who were previously diagnosed with rheumatic diseases (RD) seem to show a satisfactory level of information about their illnesses, especially those with longstanding diseases, but many of them have had incorrect beliefs, thoughts, and attitudes about rheumatology in general. Interestingly, women have a wider spectrum of knowledge about RD, probably because they have higher levels of curiosity and readiness for research and exploration [6, 7].
A lack of essential knowledge may increase patients’ concerns about the medications used in RD, which represents an essential issue regarding medication compliance and adherence. Although education may play a role, this relationship is not consistent in all cases [8, 9].
Interestingly, when attempts were made to evaluate the knowledge about rheumatology and awareness of commonly used treatment options in this field among undergraduate medical students and general practitioners in some countries, the results were disappointing. General practitioners focus mainly on subordinate aspects of the patient’s illnesses, ignoring important aspects of the patient’s care, such as disabilities that impede the provision of high-quality care. There are huge gaps not only in teaching basic information about rheumatology, but also in the up-to-date approaches and new advances in the field, as well as a significant knowledge gap in pediatric rheumatology. There is clear reluctance among medical undergraduate students to select rheumatology as a future profession after graduation [10–12].
Although it is well recognized that the most common autoimmune RD are more prevalent in women of childbearing age, knowledge about fertility, conception hazards, treatment compatibility with fetal health, and recommendations for uncomplicated and complicated labor is still limited, translating to low-quality care in this area [13].
On the other hand, gerontorheumatology (geriatric rheumatology) represents an emerging subdivision of the rheumatology specialty that can emphasize the various aspects of dealing with elderly patients with rheumatic diseases, those exceptional subgroups of patients, addressing their needs regarding diagnostic difficulties and multiple comorbidities, polypharmacy, and age-related physiological changes that impose numerous therapeutic challenges. Osteoarthritis is a key problem in the geriatric population, with a significant increase in its prevalence worldwide, exerting an enormous burden on various facets of healthcare facilities [14–16].
Rheumatic fever is another complex and illness that is somewhat confusing for the patient to understand. Despite its name suggesting a chronic traditional autoimmune condition, it is not unconditionally so; it represents a late immune reaction to group A β-hemolytic streptococcal bacterial infection that mainly involves school-age children. Again, there is a large gap in awareness regarding the various aspects of this subject [17–19].
In countries that employed media (broadcasting public campaigns), supporting groups, and public educational conferences about RD, positive results were achieved in early disease detection, scheduled early approaches, reduced financial burdens on health institutions, and outcomes in those with already established disorders, with a significant rise in public awareness, even after many years of primary events [20, 21].
Successful media-based mass education campaigns must consider society’s level of knowledge of different diseases to be valid [22].
Specifically, the disease-specific referral rate of the rheumatology clinic increased, reflecting not only an increase in public awareness about those diseases but also increased awareness among general physicians and a reduced referral threshold [23].
As many clinical, financial, social, and personal benefits were gained from increasing patients’ awareness and knowledge of their diseases, many medical societies and organizations have emphasized this aspect of patient care in their guidelines and implemented corresponding strategies [24].
This study aimed to assess the level of knowledge about rheumatology and rheumatological diseases among the general population in Basrah City and to identify the demographic, social, and educational factors associated with knowledge about rheumatology.
Material and methods
Study design
This was a cross-sectional questionnaire-based study. Participants were recruited from outpatient clinics and hospitals in Basrah City, other than rheumatology clinics. Data were collected for the period from the 1st of May 2024 to the 1st of September 2024.
The inclusion criteria were adults aged ≥ 18 years who were residents of Basrah City and expressed willingness to participate in the study. Participants were excluded if they had a known diagnosis of a rheumatological disease, were healthcare professionals, or were medical students.
The sample size was calculated through the following equation:
Sample size (N) = Z2 P(1 – P)/e2,
where: Z = Z-score (1.96 for 95% confidence level); P = expected prevalence of awareness (assumed to be 50%); e = margin of error (5%).
According to this equation, the required sample size was 385. The sample size was rounded up to 400 participants to account for potential non-responses and incomplete data.
A questionnaire was developed for the purposes of the study, which included three sections:
1. The demographic section included age, sex, educational level, residency, and occupation.
2. Subsequently, a 13-item knowledge assessment section was created after the revision of some published articles [19, 20] and discussed by two rheumatologists and a community medicine specialist. Table I presents the questions and their correct answers.
Table I
Knowledge Assessment Questionnaire
The questions covered a range of rheumatology-related diseases and were considered a core component of basic understanding in the profession.
A knowledge score was then developed. The answers to most of these questions were “yes”, “no”, and “I do not know”. Participants received 1 point for each correct answer, and zero points for the wrong answer or “I don’t know.” The sum of the correct answers was calculated and a final percentage above 50% was considered satisfactory.
3. Section three included their perception of the outcome of rheumatological diseases and the source of their information.
The questionnaire was validated through a pilot study conducted with 20 participants to assess clarity, relevance, and reliability. Cronbach’s α was calculated, and it was equal to 75%. Twenty participants included in the pilot study were excluded from the main sample.
Results
The study included 400 participants, with ages ranging from to 18 to 65 years. Fifty-six percent of them were female. Seventy-one of them had secondary school and college education, 52.5% of them were housewives and self-employed, and 70.2% of them lived in urban areas, as shown in Table II.
Table II
Demographic characteristics of participants
When testing the general knowledge about rheumatoid and rheumatological disorders in these individuals, approximately 79% of the participants stated that they had heard about these issues. Then, they were asked if they had any family member who had already been diagnosed with a RD, and 42% of the responses were positive, as shown in Table III.
Table III
Participants’ general knowledge of rheumatological diseases
| Variables | No. | % |
|---|---|---|
| Have you heard about rheumatological diseases? | ||
| Yes | 316 | 79.00 |
| No | 84 | 21.00 |
| Have any of your family members been diagnosed with rheumatological diseases? | ||
| Yes | 168 | 42.0 |
| No | 232 | 58.0 |
Table IV shows the percentage of correct answers for each question in the knowledge assessment domain. The lowest percentage of correct answers was 27% for the question “Do you think rheumatic diseases can be completely cured?” The highest percentage (50.3%) was for the question “Is rheumatoid arthritis primarily characterized by pain and stiffness in muscles and joints?”
Table IV
Percentage of participants who gave the correct answer for the knowledge assessment domain
A large percentage of the participants believed that RD could be completely cured or that they only affected the joints.
Notably, more than half of the participants had unsatisfactory knowledge (62%), and only 38% had good knowledge of rheumatology as a medical branch and the main rheumatological concepts.
Those with a satisfactory degree of knowledge about rheumatology and RD were younger than their counterparts. Moreover, 52.3% of them were female, and 47.0% had a college education. 38.8% of them were employed, and 71.1% lived in urban areas.
Analysis of this pattern demonstrated a significant association between knowledge and educational level only (p < 0.001) (Table V).
Table V
Associations between the level of knowledge and sociodemographic characteristics
About 83.4% of participants who stated that they had heard about rheumatological disease had satisfactory knowledge about the study’s domains. Contributors with a family history of RD had a better understanding of the concept of rheumatology, and this association was significant (p < 0.001). These observations are presented in Table VI.
Table VI
Associations between the level of knowledge and participants’ basic knowledge
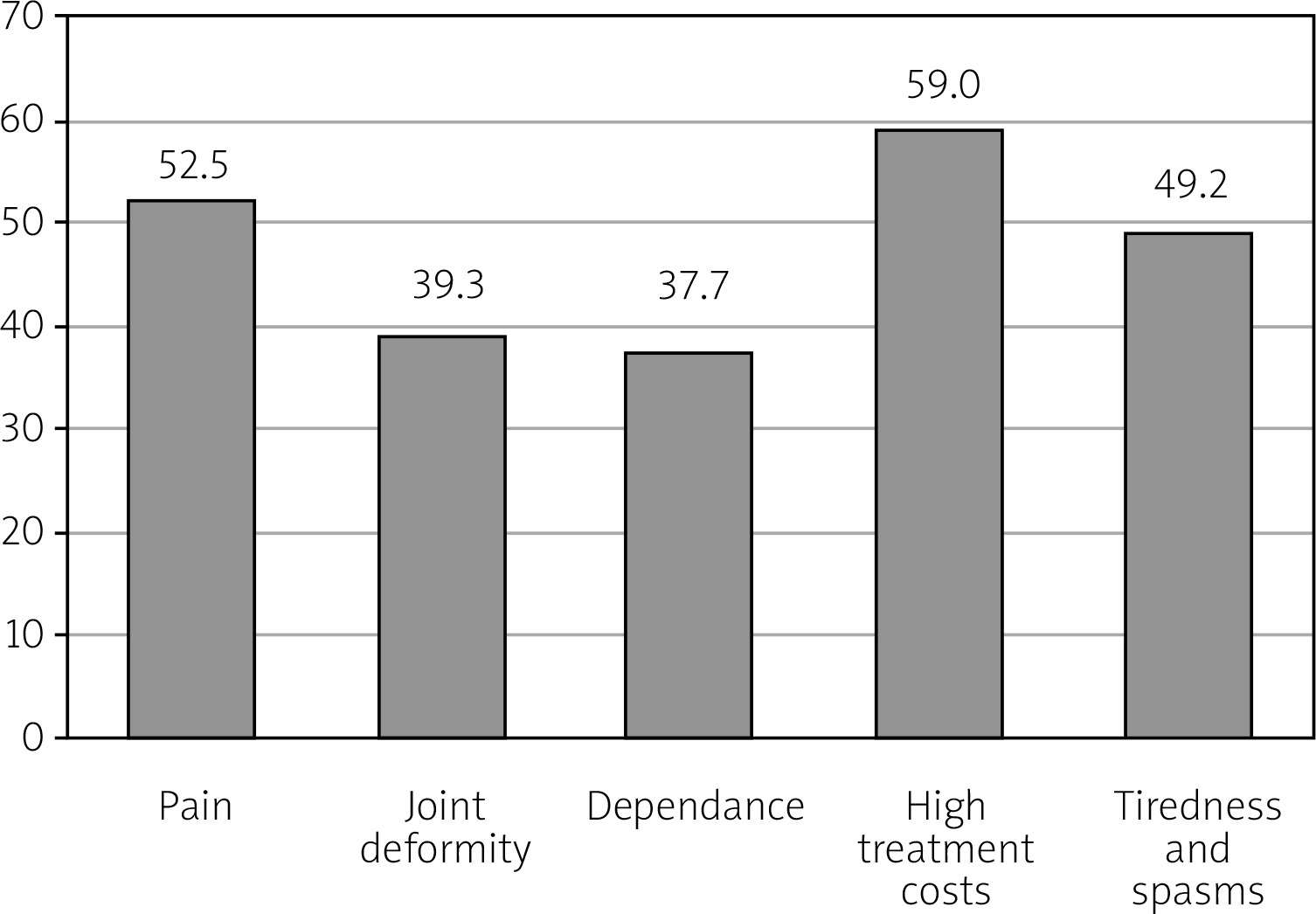
When assessing participants’ perception of the consequences of RD, about 59.0% stated that the main issue was the high cost of treatment, followed by 52.5% citing pain, and 49.2% reporting tiredness and muscle spasms, among other issues, as shown in Figure 1.
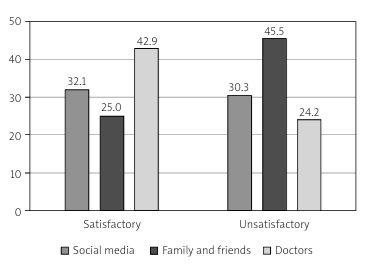
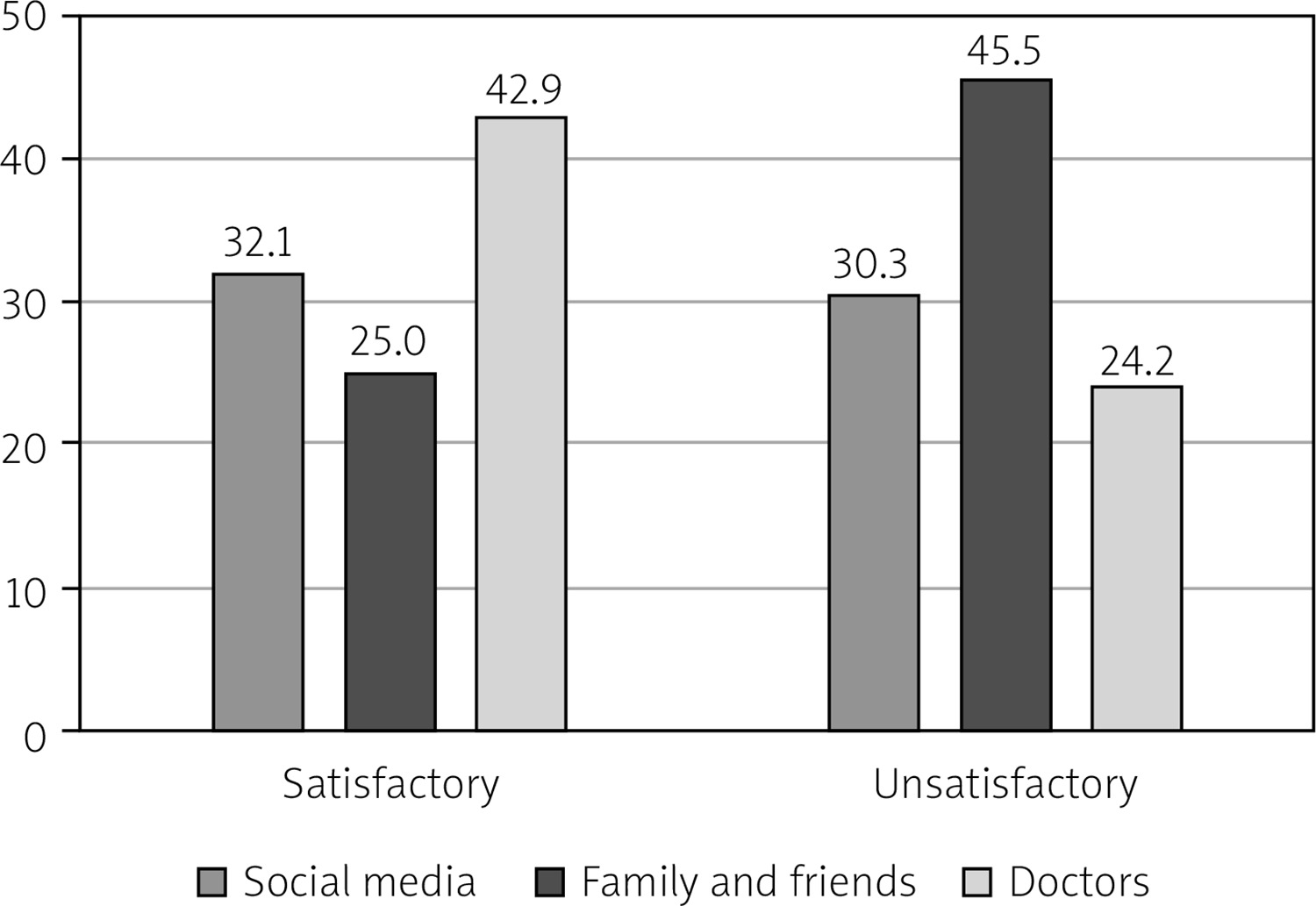
When examining sources of acquired information, doctors were cited by 42.9% of contributors with satisfactory knowledge. In contrast, in the other group, 45.5% stated that family and friends were the sources of such information. Social media were cited as the source of knowledge by one-third of the participants in the 2 groups (Fig. 2).
Discussion
In this study, most of the contributors were female, and a high percentage were young with a college education and had more curiosity to gain more evidence about concepts than those who were older and those with lower educational levels. Regarding sex, age, and academic level, our study was consistent with similar studies conducted in Poland by Pytel et al. [25] and another conducted in Saudi Arabia by Alenzi et al. [26], except that the Saudi study revealed that the level of awareness for RD was higher in men, which might be linked to social and cultural reasons.
The majority of the contributors in this study had heard about rheumatology and RD, but their level of knowledge was substandard and insufficient. Some of those with unsatisfactory knowledge had a relative affected by these disorders. This might be attributed to an insufficient number of rheumatologists, an inadequate referral system, or a lack of effective awareness campaigns.
As previously reported in several studies, and because of insufficient public knowledge about rheumatological disorders, unfavorable disease outcomes can be anticipated. For example, Danve et al. [27] reported that deficient public awareness and insufficient knowledge among non-rheumatic medical health care professionals about ankylosing spondylitis in the United States led to delayed diagnosis with poorer outcomes.
The study by Daifallah et al. [28], which was conducted in Egypt, suggested that insufficient awareness of rheumatological disorders is related to the absence of an efficient referral system accompanied by an inadequate number of rheumatologists. Consequently, some patients with these conditions consulted orthopedic surgeons and continued to visit them until adverse outcomes occurred. These factors, in turn, contributed to distorted or inaccurate perceptions of medical information about these diseases.
Clearly, and consistent with other studies, individuals who obtained a higher academic education level were more aware of the nature of rheumatic disorders and their chronic consequences for health as well as their economic repercussions for health institutions.
Our findings in this domain are consistent with Ali et al. [29], who found that educational level unquestionably and positively influences awareness of rheumatological disorders in the Syrian population.
A considerable number of the participants in this study were worried about the financial costs of treatments for rheumatological disorders; these worries are partly consistent with the situation in our local medical services and daily clinical practice because of the recurrent shortages of expensive medications used in this field. Observations such as those by Cooper [30] and Leifer et al. [31] highlighted the impact of rheumatic diseases costs on patients themselves, medical institutes, and global organizations, which is indeed substantial.
This may reflect the introduction of new treatment strategies with novel agents and multidisciplinary team approaches needed to deal with these diseases, which are generally restricted to resource-rich regions. Calderon et al. [32] estimated this burden for systemic sclerosis, which is one of the most aggressive autoimmune diseases, with high treatment and multidisciplinary team follow-up costs. Power et al. [33] highlighted the continuous financial burden of rheumatological disorders on health care institutions in Canada.
Moreover, as disease activity and severity increase, the economic cost and administrative burdens increase [34].
Another significant number of the participants in this study were concerned with the pain that may result from these illnesses, which may have a multidimensional impact, resulting in poor quality of life and individuals’ subjective performance for a considerable number of patients, even those in advanced therapeutic regimes. This is comparable to the observations of Vergne-Salleet et al. [35], who reported increased pain severity among rheumatoid arthritis patients due to psychosocial factors. The aforementioned study recommended an extended approach to detect and treat factors that may result in what seems to be a suboptimal response, even for more advanced therapies [35, 36].
In this study, other concerns regarding the long-term sequelae of RD included evolving joint deformities, muscle spasms, fatigue, and dependence on others.
Participants with good knowledge in this study gained high quality information from the doctors, which can explain the better awareness level, while those with unsatisfactory levels of knowledge gained information from their families or friends, who are likely to provide less evidence-based information. For different reasons, Van Der Wardt et al. [4] found that mass media had a negligible impact on obtaining information about RD, which is consistent with our study. This may be explained by inadequate governmental medical awareness media programs and weak mass education campaigns in our locality. In contrast to what was recognized formerly, Elsabae et al. [37] stated that the media and the Internet were the main sources of their participants’ information, followed by patients, doctors, and friends.
Conclusions
The knowledge and awareness of rheumatic diseases in our locality are deficient and limited. Misconceptions such as the belief that RD can be completely cured or that they only affect joints are not uncommon in our community. Educational level was the only factor significantly associated with satisfactory knowledge, as participants with higher educational levels were more likely to have a better understanding of RD. This highlights the critical role of education in shaping awareness and knowledge and counteracting false beliefs and irrational concerns related to rheumatological disorders. This study revealed the weak role of media and mass education campaigns in expanding awareness about these potentially serious and life-threatening disorders that can affect different ages and population groups.
Recommendations
Develop and implement targeted awareness campaigns through mass media and social platforms to educate the public about rheumatic diseases, address common misconceptions, and emphasize the importance of early diagnosis and treatment.
Encourage healthcare providers to offer informational brochures and host educational sessions targeting patients and their families in clinics and hospitals.
Encourage research to further explore public perceptions and knowledge gaps and guide the design of effective awareness strategies tailored to specific communities.
Advocate for government and non-governmental organizations to prioritize rheumatology awareness within public health agendas and allocate resources for sustained campaigns.