
Introduction
Pain is considered the cardinal symptom in rheumatology [1]. Research on the definitions, pathophysiology, classification, diagnosis, and treatment of pain is still ongoing, and international organizations, such as the World Health Organization and the International Association for the Study of Pain, have not reached a consensus on the topic. The reason is that each patient perceives pain differently and subjectively. Pain may have different components: nociceptive, neuropathic, and nociplastic [2–5].
Nociceptive pain is due to abnormal stimulation of the peripheral nociceptors with a healthy nervous system, whereas neuropathic pain is due to damage to the nervous system itself [6, 7].
Nociceptive pain is usually easily described by the patient; it is therefore quickly identified by the doctor and responds to the analgesics widely prescribed in rheumatological settings. By contrast, neuropathic pain is generally underdiagnosed [7].
This dichotomy is not always real, and in many rheumatological situations, the 2 pathophysiological mechanisms are intertwined [3, 8].
In rheumatological settings, neuropathic pain is mainly found in sciatica, root canal compression, toxic, diabetic, and drug disorders, but also in complex regional pain syndromes [9]. More recently, neuropathic pain has also been recognized as a symptom of patients with chronic inflammatory rheumatism, including rheumatoid arthritis (RA) [10]. Indeed, it has been reported that about 40% of RA patients had persistent pain during their follow-up, despite RA being clinically controlled. This suggests that the pain of RA patients may have another neuropathic component associated with the nociceptive component [11] and suggests that conventional anti-inflammatory treatment may not fully address all pain mechanisms in RA patients, highlighting the importance of screening for neuropathic features.
Neuropathic pain in RA is thought to arise from a combination of central and peripheral mechanisms. Peripheral neuropathy in RA may result from inflammation that affects nerve tissues, while central sensitization can occur due to prolonged nociceptive inputs from inflammatory processes. These 2 mechanisms contribute to the persistence of pain, even when the inflammatory activity of RA has been controlled with disease-modifying anti-rheumatic drugs (DMARDs), biologics, or glucocorticosteroids (GCs).
Recent studies have highlighted that the presence of neuropathic pain in RA may be linked to structural changes in the nervous system, including nerve fiber damage and altered pain processing pathways in the central nervous system. These changes are not always fully addressed by conventional RA treatments, which primarily target inflammation. As a result, RA patients may continue to experience significant pain despite adequate disease control, further emphasizing the need for a nuanced understanding of pain in RA that incorporates both inflammatory and neuropathic mechanisms [12]. Several studies have identified clinical tools to assess neuropathic pain in RA, further supporting the need to better understand this complex pain phenotype.
Few studies have investigated neuropathic pain in RA using standardized questionnaires, and even fewer have assessed this in North African populations. This makes our study both timely and relevant.
The aim of this study was to determine the prevalence of neuropathic pain in patients with RA and associated factors.
Material and methods
Study design
This was a cross-sectional study, including RA patients receiving care at the rheumatology department of a tertiary hospital. Patients were recruited during consultations, day hospital visits, or conventional hospitalization, between June 2023 and November 2023. All patients gave their consent prior to being included, and the study was approved by our local ethics committee.
Study population
The study included patients aged 18 years or older, diagnosed with RA according to the American College of Rheumatology/European Alliance of Associations for Rheumatology 2010 criteria [13]. Exclusion criteria were patients with impaired cognitive functions and patients followed for degenerative disorders or inflammatory pathologies other than RA.
The sample size of our study was estimated according to the Cochran formula:
n = 1.962 × p × (1 – p)/e2.
It emerged that at least 120 patients should be included for an estimated prevalence of neuropathic pain of 10% (according to a Moroccan study [14]), a confidence interval of 95%, and a risk of error of 5%. We considered the Moroccan study as a reference given our geographical and ethnic proximity.
Data collection
A questionnaire was administered to patients after their prior agreement, either by telephone or in a direct interview. The following data were collected:
epidemiological data: age, sex, body mass index (BMI), educational level, occupation, marital status, geographic origin, habits and comorbidities;
data relating to RA: age of onset, duration of progression, immunological status of RA (rheumatoid factor positivity, anti-citrullinated peptide antibodies [ACPA] positivity and the presence or absence of antinuclear antibodies) and RA activity (number of tender joints [NTJ], number of swollen joints [NSJ], C-reactive protein [CRP], Disease Activity Score in 28 joints [DAS28] and the Visual Analogue Scale of pain). Prescribed treatments: symptomatic, synthetic DMARDs, and biologic DMARDs;
data relating to the evaluation of neuropathic pain: 2 questionnaires were used:
– the PainDETECT questionnaire: a questionnaire that screens the presence of neuropathic pain. It was initially developed for patients with chronic low back pain, then extended to other pathologies. It is composed of 9 items. The score obtained is scored out of 38. A score ≥ 19 indicates probable neuropathic pain [15];
– the DN4 (Douleur Neuropathique 4) questionnaire: a simple and quick questionnaire, composed of 10 yes/no questions. Scores range from 0 to 10, with a score of 4/10 indicating neuropathic pain [16]. The questionnaire was used in its validated Arabic version [17].
Statistical analysis
Data were analyzed using SPSS Statistics software, version 27.0 (IBM Corp., Armonk, NY, USA). Continuous data were described using parametric tests. Variables following a normal distribution were presented as mean ±standard deviation. To compare 3 or more groups, one-way analysis of variance was used. Nonparametric data were presented as median and interquartile range and analyzed using the Mann-Whitney U test for comparisons between 2 groups, or the Kruskal-Wallis test for comparisons between more than 2 groups. The categorical variables were recorded as numbers (n) and percentages (%). The statistical significance level was set at p < 0.05.
Correlation and agreement between the 2 questionnaires (DN4 and PainDETECT) were estimated through Cohen’s κ (values ≤ 0 indicating no agreement, between 0.01 and 0.20: none to slight, 0.21–0.40: fair, 0.41–0.60: moderate, 0.61–0.80: almost perfect agreement).
Results
Our study was based on 121 patients with RA. The average age was 57 ±12.2 years, ranging from 20 to 81 years. Female predominance was noted (83%, n = 101).
The mean DAS28 was 4.28 ±1.00, indicating moderate activity of RA. Glucocorticosteroids, administered orally, were the most frequently prescribed symptomatic treatments (76.9%, n = 93), with an average dose of 7.5 ±1.2 mg/day. The most frequently prescribed synthetic DMARD was methotrexate (MTX; 67%), with an average dose of 10 ±2.5 mg/week.
Tumor necrosis factor inhibitors (TNFi) were the most frequently prescribed biologic DMARDs in our patients (41.3%), with infliximab being the most common (18.2%). The Table I illustrates the sociodemographic and disease characteristics of patients.
Table I
Sociodemographic and disease characteristics
[i] ACPA – anti-citrullinated peptide antibodies, AAN – antinuclear antibodies, BMI – body mass index, CRP – C-reactive protein, DAS28 – Disease Activity Score, DMARD – disease-modifying anti-rheumatic drug, DN4 – Douleur Neuropathique 4, F – female, GC – glucocorticoid, IL-6 – interleukin-6, M – male, MTX – methotrexate, NSAIDs – non-steroidal anti-inflammatory drugs, NSJ – number of swollen joints, NTJ – number of tender joints, RF – rheumatoid factor, RTX – rituximab, SD – standard deviation, VAS – Visual Analogue Scale, TNF – tumor necrosis factor
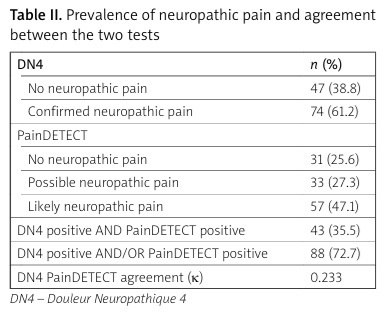
Seventy-four patients (61.2%) had confirmed neuropathic pain according to the DN4 score, and according to the PainDETECT score, 57 patients (47.1%) had likely neuropathic pain associated with RA. Eighty-eight patients (72.7%) had neuropathic pain according to the DN4 and/or PainDETECT score. The coefficient of agreement k between the 2 tests DN4 and PainDETECT was 0.233, indicating a fair agreement (Table II).
Table II
Prevalence of neuropathic pain and agreement between the two tests
Subjects with neuropathic pain (DN4 positive and/or PainDETECT positive) were more likely to be female (p = 0.01), and had a significantly higher prevalence of hypertension (p = 0.02) and osteoporosis (p = 0.04). Our results also showed a significant positive correlation of neuropathic pain with the duration of morning stiffness (p = 0.01), the mean NTJ (p = 0.01), and the mean NSJ (p = 0.03).
No statistically significant correlation was found between the presence of neuropathic pain and the mean DAS28-CRP score (p = 0.16), the mean CRP (p = 0.06), or the mean number of nocturnal awakenings (p = 0.76).
Regarding treatment, our study revealed a statistically significant association between the presence of neuropathic pain and the use of GCs (p = 0.001), the use of analgesics (p = 0.03), and the use of anti-CD20 drugs (p = 0.03).
Table III presents the comparison of sociodemographic and disease-related characteristics between patients with and without neuropathic pain, as assessed by the DN4 and PainDETECT scores.
Table III
Comparison between patients with and without neuropathic pain (according to DN4/PainDETECT scores)
[i] ACPA – anti-citrullinated peptide antibodies, AAN – antinuclear antibodies, BMI – body mass index, CRP – C-reactive protein, DAS28 – Disease Activity Score, DMARD – disease-modifying anti-rheumatic drug, DN4 – Douleur Neuropathique 4, GC – glucocorticoid, IL-6 – interleukin-6, MTX – methotrexate, NSAIDs – non-steroidal anti-inflammatory drugs, NSJ – number of swollen joints, NTJ – number of tender joints, RF – rheumatoid factor, RTX – rituximab, VAS – Visual Analogue Scale, TNF – tumor necrosis factor
Discussion
In this study, a substantial proportion of patients (72.7%) presented features suggestive of neuropathic pain in at least one of the screening tests: 61.2% according to DN4 and 47.1% according to PainDETECT. The different proportions of neuropathic pain according to DN4 and PainDETECT may be explained by different diagnostic performance of those tools. The DN4 questionnaire tends to have a high sensitivity but a low specificity to identify neuropathic pain [16]. We found a fair agreement between the 2 tests, suggesting different measurement properties of the tools.
The prevalence of neuropathic pain in our study was higher than in some previously reported studies. According to de Araújo Pereira et al. [18], in a sample of 33 patients with RA, the incidence of peripheral neuropathy according to the DN4 score was 48.5%.
The choice to use screening tools such as DN4 and PainDETECT in this study was driven by their practicality, low cost, and ability to quickly identify patients who may suffer from neuropathic pain. These tools are widely used in clinical practice and research due to their non-invasive nature and ease of administration. It is important to acknowledge that the screening tools used in this study are not gold-standard diagnostic methods. While they are sensitive, they may yield false positives or false negatives, which limits the diagnostic certainty in identifying neuropathic pain.
In our study, neuropathic pain was significantly more frequent among women (p = 0.01). This finding aligns with previous studies that have consistently reported sex-based differences in pain perception, with women experiencing pain more frequently and intensely, including neuropathic pain. Women may experience pain more frequently and may have lower thresholds or tolerance levels [9, 19], which could partly explain the higher prevalence observed in our female participants. According to a study that included 76,095 participants, female sex was associated with neuropathic pain compared to patients without chronic pain [20].
Based on the results of our study, no significant association was found between the age of RA patients and neuropathic pain. However, other studies have reported that neuropathic pain during RA is associated with young age of patients [21].
In our study, no significant association was found between BMI and the presence of neuropathic pain. However, previous studies have found that neuropathic pain was more common in individuals with an elevated BMI [21]. Indeed, obese patients are known to exhibit higher levels of inflammatory markers such as interleukin-6 (IL-6), TNF, and CRP, and proinflammatory cytokines are implicated in the development of a hyperalgesic state [22]. In addition, chronic pain can lead to a sedentary lifestyle, leading to obesity. Thus, many studies have shown that obesity and pain have a complex relationship, but the relationship between obesity and neuropathic pain remains unclear.
The lack of association between NP and BMI in our study may be attributed to population differences, as our cohort consists of North African patients, who might exhibit distinct profiles compared to other ethnic groups. Additionally, since DN4 and PainDETECT are screening tools and not gold-standard methods, their sensitivity and specificity may not fully capture neuropathic pain, potentially leading to an underestimation.
According to our results, neuropathic pain was significantly associated with comorbidities associated with RA, including hypertension (p = 0.02) and osteoporosis (p = 0.04). However, no association was noted between the presence of neuropathic pain and the duration of RA progression. The data in the literature are very controversial on this subject.
Several studies have found similar results to ours, showing that neuropathic pain can occur at any stage of RA [11, 18]. However, Filatova et al. [23] found that neuropathic pain was more common during older RA. In contrast, Martins Rocha et al. [19] reported that the duration of RA progression was inversely associated with Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) questionnaire scores.
In our study, no significant relationship was found between the presence of neuropathic pain and the immunological status of RA. In the study of Martins Rocha et al. [19], ACPA-positive patients had less neuropathic pain, as detected by the LANSS score, than ACPA-negative patients (p = 0.03). This disparity in results could be explained by differences in the properties of the screening tools used.
In accordance with previous evidence, we found that RA patients with neuropathic pain features had significantly more subjective parameters, including more prolonged morning stiffness (p = 0.01) and more NTJ (p = 0.01), but no significant association was found with objective inflammatory parameters, such as CRP, or the DAS28 activity score. This confirms the hypothesis that mechanisms independent of inflammatory activity are involved in RA chronic pain, such as deficits in central pain-processing mechanisms, inducing hyperalgesia and allodynia [24].
A significant association was found between NSJ and neuropathic pain, suggesting that ongoing joint inflammation could contribute to altered pain processing in RA patients.
Regarding RA treatments, the use of analgesics, GCs, and anti-CD20 biologics were significantly correlated with neuropathic pain (respectively p = 0.001, p = 0.03 and p = 0.03). This could be explained by the fact that patients with neuropathic pain tended to take more analgesics, believing that they would improve their pain. Nevertheless, these analgesics had no effect on this non-nociceptive component of pain.
Martins Rocha et al. [19] also found a positive association between analgesic use and the presence of neuropathic pain (p = 0.02 according to the LANSS score and p = 0.07 according to the PainDETECT score).
No significant association was found between conventional DMARDs, TNFi, anti-IL-6 and the presence of neuropathic pain in our study. However, previous studies have suggested the potentiating effect of MTX in neuropathic pain. Indeed, intrathecal injection of MTX in animal models with RA led to the worsening of neuropathic symptoms [25], although this has not been confirmed in humans [26].
Studies have also reported cases of peripheral neuropathies on leflunomide, which persisted even after discontinuation of treatment [27, 28]. Tumor necrosis factor inhibitor-induced neuropathy has also been described [29], but our study did not confirm those results.
However, our study found a significant association between the presence of neuropathic pain and the use of anti-CD20 drugs (p = 0.01). Cases of rituximab (RTX)-induced neuropathies have been reported [30]. Hypothesized mechanisms include secretion of neurotoxic autoantibodies by RTX-insensitive cell populations [31], or an RTX-induced autoimmune response resulting from disruption of the idiotype-anti-idiotype network and the production of pro-inflammatory cytokines [32].
The originality of our study lies in its use of 2 complementary screening tools to identify neuropathic pain features in a diverse RA population. Unlike many previous studies with smaller samples or single-tool assessment, we provide a broader picture of neuropathic pain prevalence and its associations in daily clinical practice. This contributes new data from a North African context, where such information remains scarce despite the high RA burden.
Study limitations
However, our study has some limitations. First, the assessment of pain was based on subjective tools that rely solely on patients’ self-reported experiences, which can vary considerably from one patient to another, and so may affect the reliability and consistency of the results. Second, although validated screening tools for neuropathic pain were used in our study, there is currently no universally accepted gold standard for its diagnosis. This may affect the accuracy and comparability of our results with other studies. Finally, the lack of data on the use of antidepressants or anticonvulsants could have influenced patients’ pain perception and their responses to screening tools.
Conclusions
Our study suggests a relatively high prevalence of neuropathic pain in RA, underlining the potential value of early screening and adequate management. Our findings support the hypothesis that neuropathic pain in RA is a multifactorial process. Thus, it requires a multidisciplinary approach and comprehensive assessment to better characterize the nature of the pain. Further research with larger sample sizes and the use of gold standard diagnostic tests, such as neurological examinations or imaging, is needed to confirm our findings. Additionally, studies exploring the impact of different RA treatments on neuropathic pain and its long-term effects on disability would be valuable. Longitudinal studies could also help clarify the relationship between neuropathic pain and disease progression in RA patients.