
Introduction
An increased risk of neoplasms in patients with autoimmune diseases has been reported in the medical literature since the 1950s. To date, numerous cohort studies have shown that the overall risk of cancers, mainly hematological ones, is elevated in this group [1]. The risk for cancers in systemic lupus erythematosus (SLE) patients is slightly elevated, with the standardized incidence ratio (SIR) estimated to be between 1.2 and 2.6, although in most studies SIR was below 2.0 [2, 3]. For comparison, after kidney transplantation in graft recipients with or without SLE, SIR was estimated to be about 3.5 [4].
Two main risk factors for neoplasm in SLE have been proposed: immune system dysregulation caused by auto immune disease, and immunosuppressive therapy [3, 5, 6]. Immune system dysfunction can explain the appearance of neoplasms in the early phase of the disease, when immunosuppressive therapy had yet not been initiated or when the duration of this treatment was short and the cumulative dose of immunosuppressant drugs was relatively low. One disturbing aspect of these cases is the risk of misdiagnosis. In fact, there are several papers describing patients with cancer in whom SLE was a misdiagnosis, or when symptoms of lupus were eventually classified as paraneoplastic syndrome [7, 8].
It has been suggested that the dysfunction of both the cellular and humoral immune systems can promote oncogenesis in SLE [3, 5, 6, 9]. However, it seems that immunosuppressive treatment is a much stronger risk factor. Drugs used in SLE treatment are well known for their oncogenic potential. For example, cyclophosphamide is responsible for the increased risk of hematological and bladder cancers, and azathioprine for non-Hodgkin lymphoma (NHL) and skin cancers [9, 10]. There is evidence of an increased risk of skin and bladder cancers after cyclophosphamide treatment in SLE patients [1, 10].
The overall risk for cancer in SLE is only slightly elevated. However, the risk of some neoplasms is much higher. In several studies, the SIR for NHL was established to be 3.5–5.5 [2, 11]. With the overall risk being slightly above 1.0 and some cancers being far more common, it is not surprising that some cancers in SLE had an SIR below 1.0.
Indeed, apart from neoplasms with SIR above 1.00 – hematological, lung, vulva, liver and thyroid cancers – there are malignancies with an incidence lower than in the general population, such as breast, endothelium, and prostate cancers [3, 11].
The risk of sarcoma in SLE is not well established. In two studies, the risk of sarcoma in SLE was high, with SIR reaching 49 and 12.1 [3, 12]. However, in these studies, the same group of 205 SLE patients (182 women and 23 men) was observed for 25 years (from 1967 to 2013) and only two cases of sarcoma were found. The authors concluded that the high SIR of sarcoma might be only “a chance finding” related to a relatively small group of subjects [3, 12].
In contrast, in several large, comprehensive studies published by Sasha Bernatsky’s group [2], the authors did not describe any case of sarcoma [2, 11, 13]. However, some evidence suggesting the possibility of sarcoma can be found in the literature. In one paper published in 2005 [2], in table 4, there is no information of sarcoma, despite the authors writing the following in the footnotes: “in addition to the categories present, the total include the following cancers: 21 non-melanoma skin […], 5 connective tissue” [2]. In a recent paper, Bernatsky et al. [1] described a group of 1,668 SLE patients with 65 cancers, which included one case of sarcoma, although no details were provided. While the SIR of sarcoma was not calculated, one case of sarcoma among 65 cancers represents a relatively high frequency.
There is no information about sarcoma in some other studies [14, 15] published from 1974 to 2013. However, scant information can be found in the discussion section of the paper by Parikh-Patel et al. [14], who noted the increased risk of bladder cancer in SLE patients and cited a paper describing leiomyosarcoma of the bladder. The 5 cohort studies or case series presenting information on sarcoma in SLE patients are listed in Table I [1, 3, 4, 12, 16].
Table I
Cohort and review studies with information about sarcoma in SLE patients
| Paper | Analyzed population | SLE patients with sarcoma | Results | Conclusions |
|---|---|---|---|---|
| Pettersson et al., 1992 Elevated risk of cancer in patients with systemic lupus erythematosus [3] | 205 patients (182 women and 23 men) with SLE treated at the Helsinki University Central Hospital from 1967 to 1987 | Two females (69 and 35 years old at the time of sarcoma diagnosis) with soft tissue sarcomas of lower limbs | 15 cancers were diagnosed against 5.7 expected (RR 2.6) There were 2 soft tissue sarcomas against 0.04 expected (RR 49) | The same group was described in 2 papers. Tallbacka et al. wrote: “The patients in our study had a statistically significant elevated risk of soft-tissue sarcoma, based on 2 observed cases. This may be a chance finding” |
| Tallbacka et al., 2018 Elevated incidence of cancer in systemic lupus erythematosus: a Finnish cohort study with more than 25 years of follow-up [12] | The same group of 205 SLE patient cohort was followed for cancer incidence from 1967 to 2013 | 45 cancers were diagnosed. An elevated risk of overall malignancy (SIR 1.90) and an elevated risk of soft-tissue sarcoma (SIR 12.1) were reported | ||
| Louthrenoo et al., 2003 Kaposi’s sarcoma in rheumatic diseases [16] | Case report and cases from a Medline search, published between 1966 and 2002 | Three cases of Kaposi’s sarcoma in SLE patients | 25 cases of Kaposi’s sarcoma reported in rheumatic diseases (11 men and 14 women) | 8 patients with rheumatoid arthritis, 5 with polymyositis/dermatomyositis, 5 with vasculitis, 3 with SLE, 2 with polymyalgia rheumatic, 1 with undifferentiated connective tissue disease and 1 with Behçet disease |
| Ramsey-Goldman et al., 2016 Standardized incidence ratios (SIRs) for cancer after renal transplant in systemic lupus erythematosus (SLE) and non-SLE recipients [4] | 143,652 renal transplant recipients with and without SLE contributed 585,420 patient years of follow-up to determine incident cancers using Medicare claim codes. From 2001 to 2009 | The risk of Kaposi’s was elevated in both groups | 10 160 cancers occurred at least 3 months after renal transplant. Overall cancer risk was increased in both SLE (SIR 3.5) and non-SLE (SIR 3.7) groups compared with the US general population | Cancer risk in renal transplant recipients was similar in SLE and non-SLE subjects, aside from melanoma. The risk of melanoma was higher in the SLE group |
| Bernatsky et al., 2021 Cancer risk in a large inception SLE cohort: Effects of demographics, smoking, and medications [1] | 1668 patients meeting ACR criteria for SLE across 33 centers (from 1999 to 2011) with an average 9 years of follow-up | One case of sarcoma | 65 cancers occurred: 15 breast, 10 non-melanoma skin, 7 lung, 6 hematological, 6 prostate, 5 melanoma, 3 cervical, 3 renal, 2 each gastric, head and neck, and thyroid, and 1 each rectal, sarcoma, thymoma, and uterine cancers | No details of a single case of sarcoma were described |
The risk of sarcoma in SLE is not well established, the main reason being its rarity and the variability of connective tissue malignancies. However, several risk factors, mainly immunosuppressive treatment, support the hypothesis that the risk of sarcoma is elevated in SLE. The medical literature features several case reports. The aim of this study was to perform a systematic review of publications describing cases of sarcoma in SLE patients.
Material and methods
To assess the risk of sarcoma in SLE patients, a systematic review on this topic was performed. The authors searched PubMed using the following terms: “(lupus or SLE or ‘lupus nephritis’) and (sarcoma or osteosarcoma or chondrosarcoma or Ewing or Kaposi or hemangioendothelioma or angiosarcoma or fibrosarcoma or myofibrosarcoma or chordoma or adamantinoma or liposarcoma or leiomyosarcoma or ‘malignant peripheral nerve sheath tumor’ or rhabdomyosarcoma or ‘malignant solitary fibrous tumor’ or dermatofibrosarcoma or ‘gastrointestinal stromal tumor’ or GIST)”.
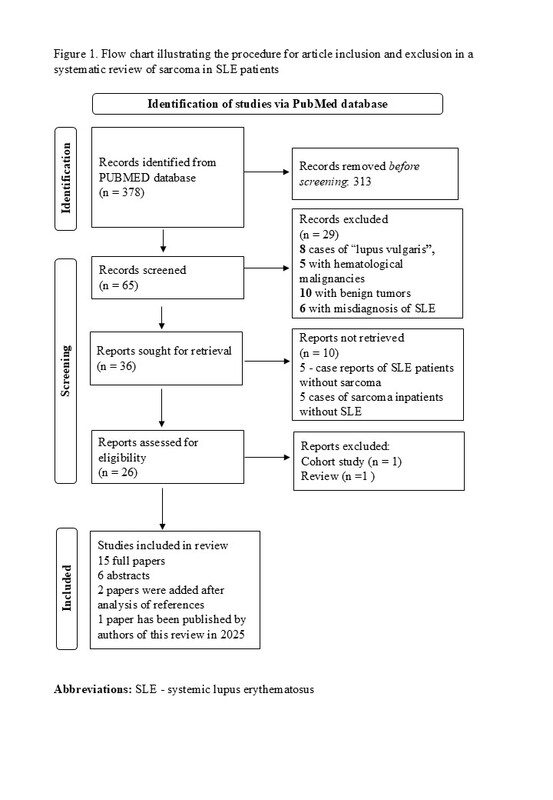
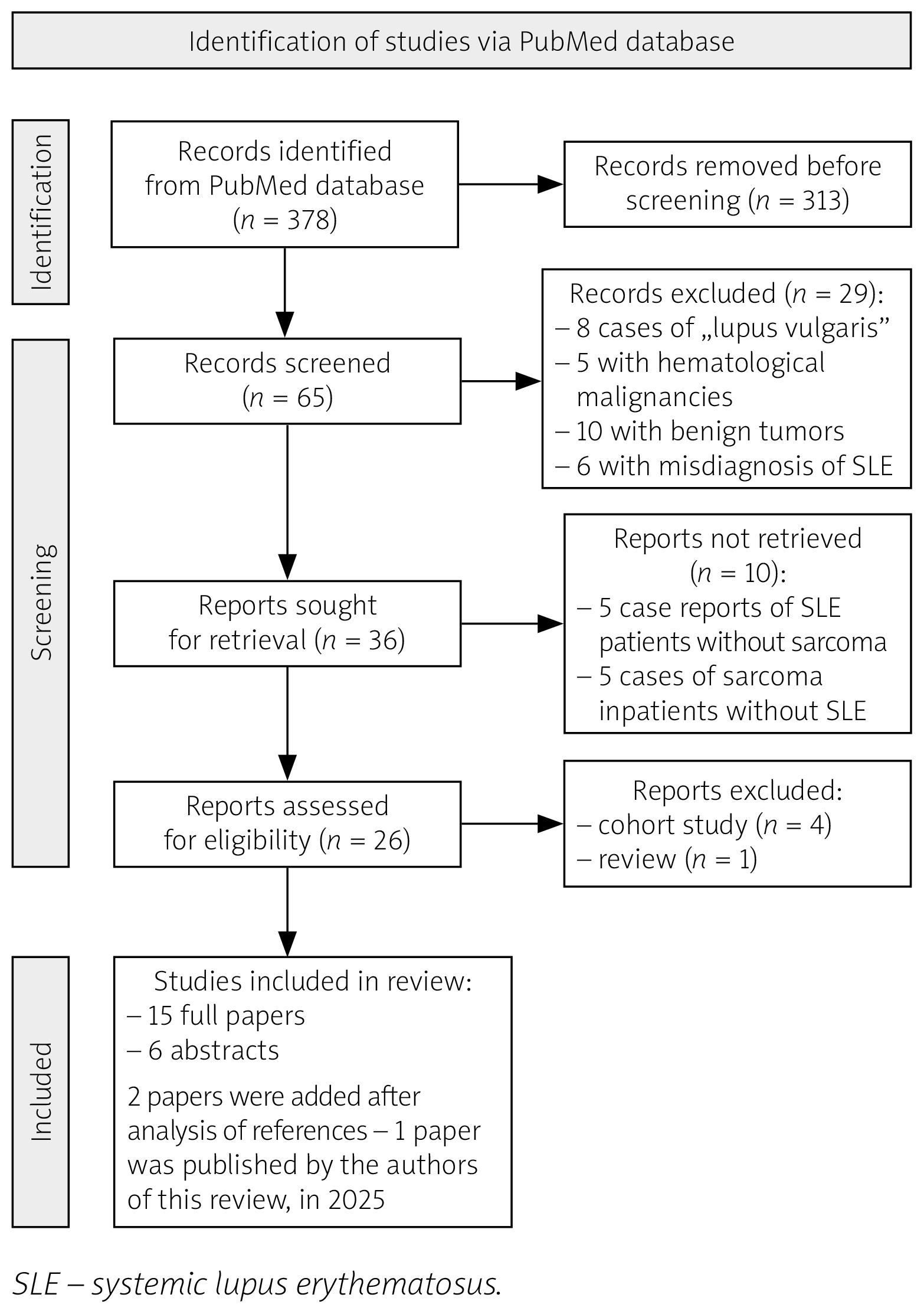
A final search was conducted in March 2025, with the aim of including recent publications. A total of 378 titles of articles published between 1947 and 2025 were found. The articles were screened first through the title and abstract; 313 records were removed before screening. We identified 65 papers for further analysis, after which 8 cases of “lupus vulgaris” were identified and excluded from the analysis, in addition to 5 with hematological malignancies, 10 with benign tumors, and 6 cases with a misdiagnosis of SLE. In 5 case reports of SLE patients, sarcoma was not confirmed, and in 5 cases of sarcoma, SLE was not confirmed; these cases were also excluded. Of the remaining 26 papers, 4 were cohort studies and one was a review (Fig. 1). Only case reports were included in the analysis.
Fig. 1
Flow chart illustrating the procedure for article inclusion and exclusion in the systematic review of sarcoma in SLE patients.
In total, 21 case reports described sarcoma in SLE patients. Fifteen full papers in English were obtained for analysis [10, 17–30]. Two additional papers were added after an analysis of the references [16, 31], and 1 was our work published in 2025 [32] (Table II).
Table II
Patients with SLE and sarcoma – full papers
| Authors, year [Ref.] | Age, sex, race or origin | SLE and co-morbidities | SLE duration before sarcoma | SLE treatment | Type of sarcoma | Area | First symptoms of sarcoma | Treatment of sarcoma | Follow-up and additional information |
|---|---|---|---|---|---|---|---|---|---|
| Klein et al., 1974 [17] | 37 years old, F, PR | SLE with LN | 3 months | P 80–60 mg/day for 3 months AZA 110–220 mg/day for 24 days | Kaposi’s sarcoma | Skin (left arm, left middle finger, both thighs) | Cutaneous nodules, lesion on the left wrist became painful | Local X-ray therapy | “Renal functions were stable, and no new lesions appeared” |
| Nikravan et al., 1983 [18] | 42 years old, M, B | SLE, gout | 19 years | P 10–35 mg/day for 13 years AZA 50 mg every other day for 8 years | Myxoid liposarcoma | Retroperitoneal space bilateral | Pain and swelling of left knee and fever | Dissection of both tumors | No information |
| Wicks and Fleming, 1986 [19] | 45 years old, F, from Greece | SLE*, scleroderma, dermato-myositis HME | 9 years | “High dose GCs” AZA CYC | Low-grade chondrosarcoma | Right calcaneum | Mass around the right ankle | No information | No information |
| Thrasher et al., 1990 [10] | 51 years old, F, W | SLE with LN, RA | 12 years | GCs CYC 100 mg/day p.o. for 12 years | Leiomyosarcoma | Bladder | Episodes of gross painless hematuria | Left partial cystectomy | The patient was free of disease 4 months postoperatively |
| Thrasher et al., 1990 [10] | 60 years old, F, W | SLE with LN, RA | 14 years | High doe GCs CYC 150 mg/day p.o. for 7 years, and 100 mg/day or 6 months | Leiomyosarcoma | Bladder | Episodes of gross painless hematuria | Total cystectomy with ileal conduit diversion | The patient was free of disease 3 years postoperatively |
| Papazisis et al., 2000 [31] | 57 years old, F, from Greece | SLE, AHA | 4 years | MP 32 mg/day | Kaposi’s sarcoma | Skin (extremities, face), soft palate mucosa | Brownish lesion on the left thigh (macular about 1 cm in diameter) | GC discontinuation | 6 months later patient had exacerbation of SLE, received IVIG and MP, 4 months later second relapse of KS |
| El Maghraoui et al., 2003 [20] | 39 years old, F, Berber | SLE with LN | 6 months | CYC 1.0 g/month i.v. for 6 months P 60–20 g/day p.o. for 12 weeks | Kaposi’s sarcoma | Skin (face, dorsum of the forearm, hands, lower legs) | Disseminated large purple nodules | Prednisone was reduced gradually to 5 mg/day | 3 months later renal function test worsened dramatically, patient died suddenly due to cardiac arrhythmia |
| Authors, year [Ref.] | Age, sex, race or origin | SLE and co-morbidities | SLE duration before sarcoma | SLE treatment | Type of sarcoma | Area | First symptoms of sarcoma | Treatment of sarcoma | Follow-up and additional information |
| Rossi et al., 2003 [21] | 18 years old, F, from Italy | SLE | 4 years | P 1 mg/kg/day gradually tapered and discontinued after 4 years | Alveolar soft part sarcoma | An irregular, solid mass of 15 mm right perirenal region, bony erosions of cranium, diffuse, round, nodular opacities in both lung fields | Dry cough, dyspnea, enlarged bilateral cervical lymph nodes | Surgical excision of the abdominal nodule, chemotherapy with vincristine, ifosfamide and carboplatin | Patient died after 6 months |
| Louthrenoo et al., 2003 [16] | 33 years old, F, from Thailand | SLE with LN and AHA DM | 8 years | High dose GCs CYC 50 mg/day (total cumulative dose 42 g) | Kaposi’s sarcoma | Skin (multiple purpuric papules and nodules on right lower eyelid, nose and left shin) | Fever, malaise, and recurrent seizures (cryptococcal meningitis was diagnosed after CSF examination) | Local radiation therapy and chemotherapy with vincristine and bleomycin | Upper gastrointestinal hemorrhage from gastric ulcers, proven to be KS; patient died 8 months later due to progressive renal and respiratory insufficiency |
| Chan et al., 2007 [22] | 24 years old, F, from Hong Kong | SLE with AHA | 4 years | High dose MP, followed by P 40–7.5 mg/day for 4 years AZA 100 mg/day for 3 years CSA 200–250 mg/ day for 5 months MMF 2 × 500 mg/day for 6 months Chlorambucil 4 mg/day for 12 months | Leiomyosarcoma | Para-umbilical mass in the abdominal wall, deep to the rectus abdominis | Ultrasound incidentally revealed a right para-umbilical mass | Radical surgery, post-operative low dose radiotherapy | There was no evidence of recurrence or metastasis 23 months after surgery; leiomyosarcoma was EBV associated |
| Authors, year [Ref.] | Age, sex, race or origin | SLE and co-morbidities | SLE duration before sarcoma | SLE treatment | Type of sarcoma | Area | First symptoms of sarcoma | Treatment of sarcoma | Follow-up and additional information |
| Hoene et al., 2008 [23] | 27 years old, F, B | SLE | “Long history of lupus” | No information | Inflammatory myofibroblastic tumor | Large left-sided bladder mass | Fatigue, fever, diffuse myalgia, weight loss Occasional urinary obstructive symptoms | Radical cystectomy with ileal conduit | No clinical or radiologic evidence of recurrence for 6 months |
| De la Pena and Wapnir, 2008 [24] | 50 years old, F, from USA | SLE, RA, DM, asthma | 10 years | CYC exposure was intermittent over 10 years Zafirlukast Fluticasone | Leiomyosarcoma | Left breast | Patient detected a mass in her left breast on self-exam | Mastectomy | No evidence of recurrent disease 11 months after mastectomy |
| Baydar et al., 2009 [25] | 24 years old, F, from Turkey | SLE | 13 years | P 10–32 mg/day for 12 years AZA 100 mg/day for 3 months HCQ 400 mg/day for 10 years CYC 50–150 mg/day for 10 years | Osteosarcoma | Bladder | Left flank pain and hematuria | Radical cystectomy with ileal conduit urinary diversion | No evidence of recurrence or metastasis 6 months after surgery |
| Oliveira and Martins, 2012 [26] | 39 years old, F, from Brasil | SLE | 19 years | No information | Malignant fibrohistocytoma | Left tibia | Pain in the left ankle | Radical resection of lesion | Without recurrence at 5-years follow-up |
| Jia et al., 2013 [27] | 46 years old, F, from China | SLE | 2 years | P 10 mg/day for 2 years | Undifferentiated embryonal Sarcoma | Right lobe of the liver | Upper abdominal pain | Segmentectomy of S5 and S4a and cholecystectomy | At the 6-month follow-up, an unresectable tumor was detected; the patient died one year later |
| Chen et al., 2014 [28] | 31 years old, F, from Taiwan | SLE with LN | 9 years | “Mainly” P 10–20 mg/day for 9 years | Kaposi’s sarcoma | Skin (right anterior nasal floor near the nostril) | Swelling and bulging nodule of the right side of nose | Local excision and low dose radiation therapy | No recurrence during the four years of follow-up |
| Authors, year [Ref.] | Age, sex, race or origin | SLE and co-morbidities | SLE duration before sarcoma | SLE treatment | Type of sarcoma | Area | First symptoms of sarcoma | Treatment of sarcoma | Follow-up and additional information |
| Khan et al., 2014 [29] | 40 years old, F, from UK | SLE and APS | No information | HCQ | Leiomyosarcoma | Retroperitoneal space | Left-sided loin pain | Laparoscopic adrenalectomy and radiotherapy | Subject survived for well over 60 months |
| Ritter et al., 2024 [30] | 39 years old, F, from Israel | SLE and APS | 8 years | HCQ for 8 years P 20 mg/day for 8 months MTX 15 mg/week for 8 months Belimumab 200 mg/week for 8 months | Spindle cell sarcoma | Left atrium | Clubbing of fingers and toes | Mitral valve replacement, the second surgery with excision of large gelatinous, encapsulated mass Chemotherapy (adriamycin and ifosfamide) and radiotherapy | Patient had a good response, the digital clubbing had partly regressed |
| Malinowski and Wołyniec, 2025 [32] | 42 years old, F, W | SLE with LN | 8 years | GCs CYC (6.0 g), AZA, MMF, CSA HCQ | Dermatofibro-sarcoma | Left breast | Patient detected a mass in her left breast on self-exam | Radical surgery | No recurrence during the 5 years of follow-up |
| Malinowski and Wołyniec, 2025 [32] | 30 years old, F, W | SLE with LN | 14 years | GCs CYC (2.3 g), MMF HCQ | Giant cell tumor | Left femur | Pain in the left thigh | Radical surgery | After 1 year new lesions in left femur were detected; patient died suddenly at home |
* The first diagnosis was dermatomyositis; after 3 years of treatment the patient was lost to follow-up for 7 years; eventually, SLE and scleroderma were diagnosed. AHA – autoimmune hemolytic anemia, AZA – azathioprine, B – Black or African American, CSA – cyclosporine, CYC – cyclophosphamide, DM – diabetes mellitus, EBV – Epstein-Barr virus, F – female, GCs – glucocorticosteroids, HCQ – hydroxychloroquine, HME – hereditary multiple exostoses, i.v. – intravenous, KS – Kaposi’s sarcoma, LN – lupus nephritis, M – male, MP – methylprednisolone, MMF – mycophenolate mofetil, MTX – methotrexate, P – prednisone, p.o. – per os, PR – Puerto Rican, RA – rheumatoid arthritis, SLE – systemic lupus erythematosus, W – white.
Altogether, 20 patients were described in 18 full papers written in English. We also analyzed 6 cases described in abstracts [33–38], when the full paper was not written in English or when the full paper was not found but basic information could be obtained from the abstract (Table III).
Table III
Patients with SLE and sarcoma – abstracts
| Authors, year [Ref.] | Age, sex, race or origin | SLE andco-morbidities | SLE duration before sarcoma | SLE treatment | Type of sarcoma | Area | First symptoms of sarcoma | Treatment of sarcoma | Follow-up and additional information |
|---|---|---|---|---|---|---|---|---|---|
| Greenfield et al., 1986 [33] | 31 years old, F | SLE | ND | CS | Kaposi’s sarcoma | Skin and lung | ND | ND | Died |
| Tamura et al., 1987 [34] | 24 years old, F | SLE | At least 5 years | P 7–40 mg/day for 5 years | Angiosarcoma | Right breast | ND | Radical mastectomy and adjuvant chemotherapy with actinomycin D | The patient remained well 26 months after the operation |
| Fyfe et al., 1991 [35] | 46 years old, F | SLE | ND | ND | Leiomyosarcoma | Left atrium | Symptoms and signs of rapidly progressive left ventricular failure | Surgical | Died 7 months postoperatively |
| Fagone et al., 2001 [36] | 78 years old, F | SLE | At least 10 years | Long period of a low-dose CS | Kaposi’s sarcoma | Skin (right leg and foot) | Red-blue multiple hyperkeratotic nodules | ND | ND |
| Ashfag et al., 2004 [37] | 28 years old, F | SLE with LN KTx | 26 months post transplantation | ND | Leiomyosarcoma | Renal allograft | ND | ND | ND |
| Kim et al., 2009 [38] | 42 years old, F | SLE | ND | ND | Kaposi’s sarcoma | Gingiva | Gingival hyperplasia | Excision and chemotherapy | ND |
Results
Twenty cases described in detail in 18 full papers were analyzed [10, 16–32]. Information covering an additional 6 cases was found only in abstracts (full papers were not written in English or were not available) [33–38]. The information from abstracts was scarce, although the essential data about age, sex of patients, and the type of sarcoma and its location were found.
All patients except 1 [18] were females, originating from different countries and continents. There was no precise information about racial and ethnic predominance. The mean age of all 26 patients at the time of sarcoma diagnosis was 39.35 ±13.2 years; the youngest patient was 18 [21], and the oldest 78 years of age [36].
The most common diagnosis was Kaposi’s sarcoma, representing 30.8% (8/26) of all sarcomas [16, 17, 20, 28, 31, 36, 38], followed by 7 leiomyosarcomas (26.9% of all sarcomas) [10, 22, 24, 29, 35, 37]. The remaining 11 sarcomas were represented by single cases, showing the huge variety of connective tissue neoplasms.
The skin was the organ most frequently involved, and 7 patients had Kaposi’s sarcoma of the skin. In 4 patients, sarcoma was located in the bladder, and at least 3 of these patients had been treated with cyclophosphamide before the sarcoma diagnosis [10, 25]. In 1 case, there was no information about immunosuppression. Three sarcomas were located in bones (calcaneum, tibia and femur), 3 in the breast, 2 in the mucosa, 2 in the retroperitoneal space, and 2 in the left atrium. Moreover, there were single cases of sarcoma of the abdominal wall, liver, and renal allograft. In 1 case, the disease was disseminated at the time of diagnosis.
In 18 cases, information regarding the duration of SLE before sarcoma was available, and this ranged from 3 months to 19 years (mean 9.07 ±5.36 years).
The immunosuppressive regimens varied substantially, reflecting the progress that was achieved in SLE treatment over a period of half a century. The early cases were treated with glucocorticosteroid, azathioprine, and cyclophosphamide; the last patients were receiving hydroxychloroquine, methotrexate, mycophenolate mofetil, and belimumab.
In 15 out of 19 cases, surgery was the main treatment. Radiotherapy was the only treatment in 1 case, and adjuvant in 5 others. Chemotherapy was used in 3 cases but never as the sole treatment. Glucocorticosteroid discontinuation or reduction was used in 2 Kaposi’s sarcoma patients. This approach leads to a short-term improvement, but in the follow-up a relapse of SLE and recurrence of sarcoma were observed. There is information about 7 deaths in 21 cases (in 5 cases, the follow-up was not mentioned). The follow-up after sarcoma treatment ranged from 4 to 60 months; consequently, the real mortality is difficult to establish.
Discussion
Sarcomas are heterogeneous malignancies of connective tissue. The systematics of sarcoma is difficult, with this field being generally divided into two groups: bone and soft tissue sarcomas. Primary bone sarcomas account for less than 0.2% of malignant neoplasms across all ages. The overall incidence rate ranges between 0.8 and 0.9 cases per 100,000/year. The most common bone sarcomas are osteosarcoma and Ewing sarcoma. Some neoplasms, such as giant cell tumors of bone, are only locally aggressive and rarely metastatic [39]. The incidence of soft tissue sarcomas in adults in Europe is approximately 4–5 cases per 100,000/year, with the average age of diagnosis being 59 years. The most common are leiomyosarcoma and liposarcoma [40].
Sarcomas represent 1% of all cancers. This rarity makes it difficult to calculate the risk in patients with SLE. Well-known risk factors for sarcomas are exposure to various chemicals and ionizing radiation [39, 40]. Patients with SLE are generally more exposed to both these factors, yet immunosuppressive drugs seem to be the most important risk factor.
Exposure to immunosuppression is a well-known risk factor for cancers [3, 5, 6]. All the patients described above received some immunosuppressive medication, although this was administered in different regimens with different durations and various doses. It is impossible to assess which treatment was the most harmful, if any. However, not only drugs but also the disease itself lead to immune system dysfunction. The impact of immune dysfunction on the risk for sarcoma could not be assessed on the basis of case reports. In our review, at least seven sarcomas were diagnosed in the first 5 years of SLE treatment [17, 20–22, 27, 31, 34]. However, the majority of cases were diagnosed in patients with a much longer history of immunosuppressive treatment.
In patients with neoplasms diagnosed shortly after the onset of SLE, the possibility of misdiagnosis should be taken into consideration. The literature features cases of angiosarcoma [8] and primary sarcoma of the heart [41] mimicking lupus. In 1 case presented in our review, Kaposi’s sarcoma was diagnosed only 3 months after SLE onset. In this case, there was no doubt about SLE diagnosis, as the patient presented typical symptoms, laboratory abnormalities, and an immunological test, resulting in lupus nephritis being confirmed by kidney biopsy [17].
Interestingly, the first cases of sarcoma following lupus were published several years before azathioprine was synthesized in 1957. Unfortunately, only the titles of papers written by Kopf in 1947 [42] and Winkle in 1950 [43] were available for the authors of this review; therefore, no information of the treatment of these patients was found.
In 1904, many years before modern immunosuppressive therapy, Perthes described a case of a spindle cell sarcoma that followed radiation therapy for lupus, which was one of the first cases of a neoplasm after radiotherapy [44]. The harmful effect of ionizing radiation is a well-recognized risk factor for neoplasms. However, it was impossible to provide even a rough estimate of the radiation dose in patients described in case reports, although it is clear that SLE patients underwent more imaging studies in their life than healthy ones.
One very interesting problem is the impact of viral infection. In this review, 30.8% of patients had Kaposi’s sarcoma and 26.9% had leiomyosarcomas. Kaposi’s is an extremely rare neoplasm, but is a typical cancer of immunocompromised patients, strongly related to viral infection caused by human herpesvirus 8 (HHV-8). In 2003, Louthrenoo et al. [16] described cases of Kaposi’s sarcoma in rheumatoid diseases. Twenty-five cases were reported (11 men and 14 women); 8 patients had rheumatoid arthritis (RA), 5 had polymyositis/dermatomyositis, 5 had vasculitis, 3 had SLE, 2 had polymyalgia rheumatica, 1 patient had a case of undifferentiated connective tissue disease, and 1 had Behcet’s disease.
Leiomyosarcoma, on the other hand, is one of the most common sarcomas. Therefore, it is not surprising that it was also the second most common in the present review. It is, however, important to note that this sarcoma could also be related to viral infection caused by the Epstein-Barr virus (EBV). Epstein-Barr virus is a life-long asymptomatic infection carried by the vast majority of individuals in all human populations. Epstein-Barr virus infection is associated with hematological (Hodgkin lymphoma, Burkitt lymphoma, diffuse large B cell lymphoma, plasmablastic lymphoma and primary effusion lymphoma) and solid (nasopharyngeal carcinoma, gastric carcinoma, leiomyosarcoma) malignancies [45]. In 2007, Chan et al. [22] precisely described a relationship between EBV infection and leiomyosarcoma in a patient with SLE, but this approach is uncommon, and in most cases of leiomyosarcoma there is no information about any viral infection.
The problem with virus-related neoplasm in immunocompromised patients is an interesting issue. In patients with SLE, there is a higher risk of hematological, lung, vulva, liver and thyroid cancers [3, 11], which is probably related to viral infections. Human papillomavirus infection is related to vulva and cervical cancers, EBV to hematological and leiomyosarcoma, and HHV8 to Kaposi’s sarcoma [46]. Dreyer et al. [15] described 61 malignancies in an SLE population and estimated that 29 (47.5%!) were “potentially associated” with viral infection. However, no subject had sarcoma.
Latent viral infection in patients treated with immunosuppression seems to be the main risk factor of sarcoma in SLE.
The cancers with low SIR in SLE are not related to viral infection but are hormone-dependent: the risk of breast, endothelium, ovarium, and prostate cancers is relatively low in SLE [3, 11].
The role of an immune dysfunction in sarcoma development is difficult to estimate. It could, however, explain the occurrence of sarcoma in patients treated with various regimens for various periods of time. It is also not surprising that several cases of sarcoma have been described in patients with other connective tissue diseases, such as discoid lupus erythematosus [47], Sjögren’s syndrome [32], antiphospholipid antibody syndrome [48] and RA [16].
Conclusions
Patients with SLE have an elevated risk of cancer compared to the general population. The risk of sarcoma is difficult to calculate, because both conditions – SLE and sarcoma – are relatively rare. Thus far, no direct relationship between sarcoma and SLE has been established. The development of large databases of rheumatological diseases and their analysis based on artificial intelligence may in the future enable estimation of the risk of coexistence of these two rare diseases.
Indeed, immune system dysfunction caused by autoimmune disease and immunosuppressive drugs and exposure to ionizing radiation are risk factors for occurrence of sarcoma in the SLE population. The newer therapies are safer than those used several years ago, and the availability of imaging studies makes it easier to perform them in patients with chronic diseases such as SLE. Modern immunosuppression and limitation of imaging studies seem to the best means of prophylaxis of sarcoma.
There is no good screening for sarcoma. The most common sarcoma in SLE is Kaposi’s sarcoma of the skin. An examination of the patient’s skin is essential. Also, it is important not to ignore any tumors and bumps reported by the patient.
Another interesting issue concerns the relationship between viral infection and sarcoma. In the future, new vaccines and new antiviral drugs will probably change the epidemiology of cancers in immunocompromised patients.