

Introduction
Involvement of the temporomandibular joint (TMJ) is a common yet frequently underdiagnosed manifestation of juvenile idiopathic arthritis (JIA). This condition may occur alongside arthritis in other synovial joints or, in some instances, present as the initial or sole indicator of the disease [1–4]. The reported prevalence of TMJ involvement varies widely, from 17% to over 90%, depending on the diagnostic criteria, imaging methodologies, duration of the disease, and characteristics of the patient population [1, 5–9]. A significant challenge in diagnosing TMJ arthritis lies in its subtle and often asymptomatic onset. Early inflammation typically does not exhibit clear clinical signs, and considerable structural damage can occur without any noticeable symptoms. Pain, crepitus, or functional limitations usually arise only in the later stages of the condition. Research indicates that objective indicators, such as reduced maximal mouth opening (MMO), mandibular deviation during movement, and facial asymmetry, can be present even in the absence of pain [6, 7, 10–15]. Moreover, radiologic evidence of TMJ involvement has been identified in many asymptomatic patients [9, 16].
The anatomical features of the TMJ highlight the necessity for early detection. The mandibular condyle acts as a critical growth center and is situated close to the synovial membrane. Chronic inflammation in this region can hinder growth and remodeling, leading to complications such as dentofacial asymmetry, retrognathia, anterior open bite, and long-term functional disability. These issues may develop during crucial phases of craniofacial development, significantly impacting the child’s quality of life [12, 14, 16, 17].
Magnetic resonance imaging (MRI) is regarded as the gold standard for identifying early synovial inflammation; however, it is frequently underutilized due to challenges such as limited access, high costs, and the necessity for sedation in young children [4]. In this context, early clinical indicators – such as restricted mandibular mobility, facial asymmetry, and deviation upon mouth opening – are becoming increasingly significant for diagnosis. Structured clinical examination protocols, such as the Clinical Orofacial Examination proposed by Stoustrup et al. [18], have been developed to enhance early detection.
The distinctiveness of this case-based review lies in its emphasis on subtle morphofunctional signs, particularly facial asymmetry and limited mandibular mobility, as early indicators of TMJ arthritis, developed in accordance with the “CAse-BAsed REview sTandards (CABARET): Considerations for Authors, Reviewers, and Editors” [19]. By integrating current literature with a representative clinical case, this review seeks to raise awareness of early-stage TMJ involvement, promote timely imaging, and support the establishment of standardized diagnostic pathways. Early identification and intervention are crucial for preventing irreversible damage and maintaining both function and facial symmetry in children with JIA.
Methods
This case-based narrative review was undertaken to contextualize the presented clinical case by synthesizing current evidence on the clinical and imaging manifestations of TMJ involvement in JIA. The aim of the literature component is to highlight diagnostic challenges and variability in clinical presentation, as well as to identify patterns relevant to early detection and assessment, in light of the case under discussion. A structured literature search was conducted in PubMed (MEDLINE), Scopus, and Web of Science to retrieve relevant original studies published up to June 2025. The search combined key words and medical subject headings such as: “juvenile idiopathic arthritis,” “temporomandibular joint,” “TMJ,” “arthritis,” “facial asymmetry,” “mandibular mobility,” and “CBCT.” Boolean operators (AND, OR) were used to refine the search strategy.
Inclusion criteria: 1) original studies involving JIA patients; 2) clinical and/or radiological assessment of TMJ involvement; 3) study populations with participants under 20 years of age; 4) full-text availability in English.
Exclusion criteria: 1) narrative or systematic reviews, meta-analyses, editorials, and conference abstracts; 2) studies exclusively involving adult populations (≥ 20 years); 3) research unrelated to TMJ arthritis in JIA.
After conducting an initial literature search and thoroughly reviewing available publications, a total of 30 studies [1–4, 6, 7, 9–17, 20–34] were included in this narrative synthesis. The selection process was carried out independently by the sole author, focusing on the relevance of the studies to the clinical case presented, as well as the availability of detailed clinical and/or radiological data on TMJ involvement in JIA. Publications that emphasized morphofunctional assessment, imaging findings, facial asymmetry, mandibular growth disturbances, and functional limitations were prioritized. Additionally, the reference lists of all selected studies were reviewed to identify further relevant publications using a snowballing approach; however, this strategy did not yield any additional eligible articles.
Although the methodology was not systematic in the formal sense, efforts were made to ensure transparency and completeness. No formal risk-of-bias assessment was conducted, in keeping with the narrative character of the review; however, care was taken to select studies that represent a range of clinical presentations and diagnostic methods relevant to the case scenario.
Literature review
Temporomandibular joint arthritis is a common but often underrecognized complication of JIA, with potential consequences for both functional abilities and craniofacial development. The onset of TMJ involvement is frequently gradual and asymptomatic, making early detection particularly challenging. This literature review synthesizes comparative evidence on the early signs, diagnostic tools, and clinical significance of TMJ arthritis in children with JIA, with the aim of supporting early recognition and multidisciplinary management [1, 3, 5–9].
Clinical symptoms alone are inadequate for reliably detecting TMJ involvement in JIA. While some patients report pain or masticatory difficulties, others remain asymptomatic despite significant joint pathology. Savioli et al. [13] demonstrated TMJ dysfunction in 94% of JIA patients using the Helkimo Index, with nearly half categorized as having moderate to severe dysfunction (grade II or III), whereas only 30% of them reported mild symptoms (grade I). Mohamed et al. [28] reported TMJ-related symptoms in 35% of JIA patients, including pain in 17.5%, crepitus in 7.5%, and clinical signs in 62%, with reduced MMO being the most common sign (25%). Leksell et al. [14] observed pain at rest in 22% of patients, pain during chewing in 71%, and pain during mouth opening in 68%, with reduced MMO present in 32% of cases. Similar findings were reported by Pawlaczyk-Kamieńska et al. [15], who noted reduced MMO in 58% of JIA patients with unilateral TMJ arthritis.
Despite the growing recognition of MMO as a potential clinical marker, studies by Stoll et al. [12] and Koss et al. [21] found no significant difference in MMO between JIA patients with and without TMJ arthritis, suggesting limited diagnostic specificity. However, Collin et al. [29] identified TMJ deformities in 39% of JIA patients using cone-beam computed tomography (CBCT). These structural changes were significantly associated with reduced MMO. Similar conclusions were drawn by Pawlaczyk-Kamieńska et al. [15], who observed that reduced MMO was frequently associated with radiographic abnormalities on CBCT, even in patients without overt clinical symptoms. The authors [15, 29] proposed that an MMO of less than 40 mm may serve as a sensitive clinical marker of structural TMJ involvement.
Keller et al. [24] reported facial asymmetry in 37–41% of JIA patients, more frequently than in healthy controls. In the study by Pawlaczyk-Kamieńska et al. [15], facial asymmetry was observed in 23% of patients. Keller et al. [24] also noted mandibular deviation during mouth opening in up to 62% of JIA patients, compared to only 16% in controls. Pawlaczyk-Kamieńska et al. [15] found deviation exceeding 2 mm in 46.15% of patients, most often directed toward the more affected joint. It is noteworthy that these findings were based on a cohort with confirmed unilateral TMJ arthritis.
Both studies conducted by Collin et al. [29] and Pawlaczyk-Kamieńska et al. [15] revealed strong associations between mandibular deviation, facial asymmetry, and the severity of radiographic changes. The deviation was typically directed toward the more affected joint, and an earlier onset of the disease was associated with greater restriction of lateral movement toward the contralateral, less affected side. These findings are consistent with the hypothesis that unilateral TMJ involvement disrupts symmetrical mandibular growth, potentially leading to ramus shortening and asymmetry in the lower third of the face. Pawlaczyk-Kamieńska et al. [15] further demonstrated the diagnostic value of functional assessment. A statistically significant relationship was found between facial asymmetry and mandibular deviation during mouth opening. The direction of both the mandibular and chin deviations corresponded to the side with more pronounced radiographic damage. A strong correlation was also observed between the age at disease onset and reduced lateral movement toward the less affected joint, while no association was identified with disease duration. Additionally, a positive correlation was noted between MMO and mandibular protrusion, with lateral movement significantly reduced toward the more severely affected side.
Interestingly, in the study by Pawlaczyk-Kamieńska et al. [15], no direct association was found between the severity of condylar damage and clinical symptoms. Some patients with substantial radiographic deformities were asymptomatic, while others with only mild structural changes exhibited functional impairment. The authors suggested that these observations indicate that TMJ involvement in JIA results from a complex interplay of factors, including growth disturbances, malocclusion, mechanical overload, and neuromuscular adaptation. Moreover, the severity of dentofacial deformity appears to be influenced by the age at which the disease begins, with an earlier onset associated with more pronounced mandibular growth disturbances.
While CBCT is widely used to assess bony changes such as condylar flattening, erosions, or asymmetry, it does not detect active inflammation [11, 17]. Magnetic resonance imaging remains the gold standard for the early diagnosis of TMJ involvement, as it enables detailed visualization of synovial inflammation, joint effusion, pannus formation, and bone marrow edema [4, 9, 21, 25]. Detection rates of TMJ involvement on MRI have been reported to be up to 80% in studies by Müller et al. [30] and Weiss et al. [9]. Moreover, MRI allows for differentiation between active and chronic disease, thereby supporting early and targeted therapeutic decision-making. Nevertheless, MRI access is limited in some clinical settings, and sedation may be required for younger children. Therefore, CBCT remains a valuable alternative for assessing long-term structural damage of the TMJ, particularly in patients presenting with craniofacial asymmetry or clinical suspicion of growth disturbances. Cone beam computed tomography provides high-resolution imaging of osseous structures with relatively low radiation exposure, and is especially useful in detecting condylar deformities, erosion, flattening, or asymmetry that may indicate previous inflammatory activity [31, 35]. It is considered the modality of choice when evaluating chronic, structural, or developmental abnormalities of the TMJ, especially when MRI is contraindicated or unavailable.
Ultrasound (US) has been investigated as a non-invasive and cost-effective imaging modality for TMJ assessment; however, reported diagnostic performance has been inconsistent. Jank et al. [27] demonstrated that disc displacement could be visualized in 55.5% of examined TMJs using conventional US. Nonetheless, several studies – including that by Weiss et al. [9] – have reported low sensitivity of US, particularly in the early or mild stages of TMJ arthritis. High-resolution ultrasound (HR-US), as shown by Assaf et al. [33], provides enhanced visualization of synovial width and condylar surface irregularities, offering potential advantages over standard US. Tonni et al. [34] reported promising correlations between HR-US measurements, particularly of the lateral periarticular space, and MRI findings indicative of TMJ inflammation in patients with JIA. Despite these advances, systematic reviews continue to highlight the limited sensitivity of HR-US for detecting early synovitis, as well as significant heterogeneity in imaging protocols, which currently preclude its widespread adoption in routine clinical monitoring of TMJ involvement in JIA.
To address diagnostic variability, Stoustrup et al. [18] proposed the Clinical Orofacial Examination (COFE), a standardized protocol for assessing maximum mouth opening, lateral excursions, pain on palpation, joint sounds, and facial asymmetry. Incorporation of such tools into routine rheumatologic care may improve early detection and clinical consistency across disciplines.
As an illustration of the problem, the course of the disease in a 9-year-old child is described below.
Case description
A 9-year-old girl with a 5-year history of polyarticular JIA was referred to the dentist for evaluation regarding potential involvement of the TMJ. Importantly, both the patient and her caregivers reported no symptoms related to the TMJ, including pain at rest, during mastication, or with jaw movement. Additionally, there was no history of jaw trauma, orthodontic treatment, or masticatory dysfunction. Written informed consent for participation in the study and publication of the case details was obtained from the patient’s legal guardian. The study protocol was approved by the Ethical Committee of the Poznan University of Medical Sciences (No. 1255/18) and was conducted in accordance with the Declaration of Helsinki and local bioethics regulations.
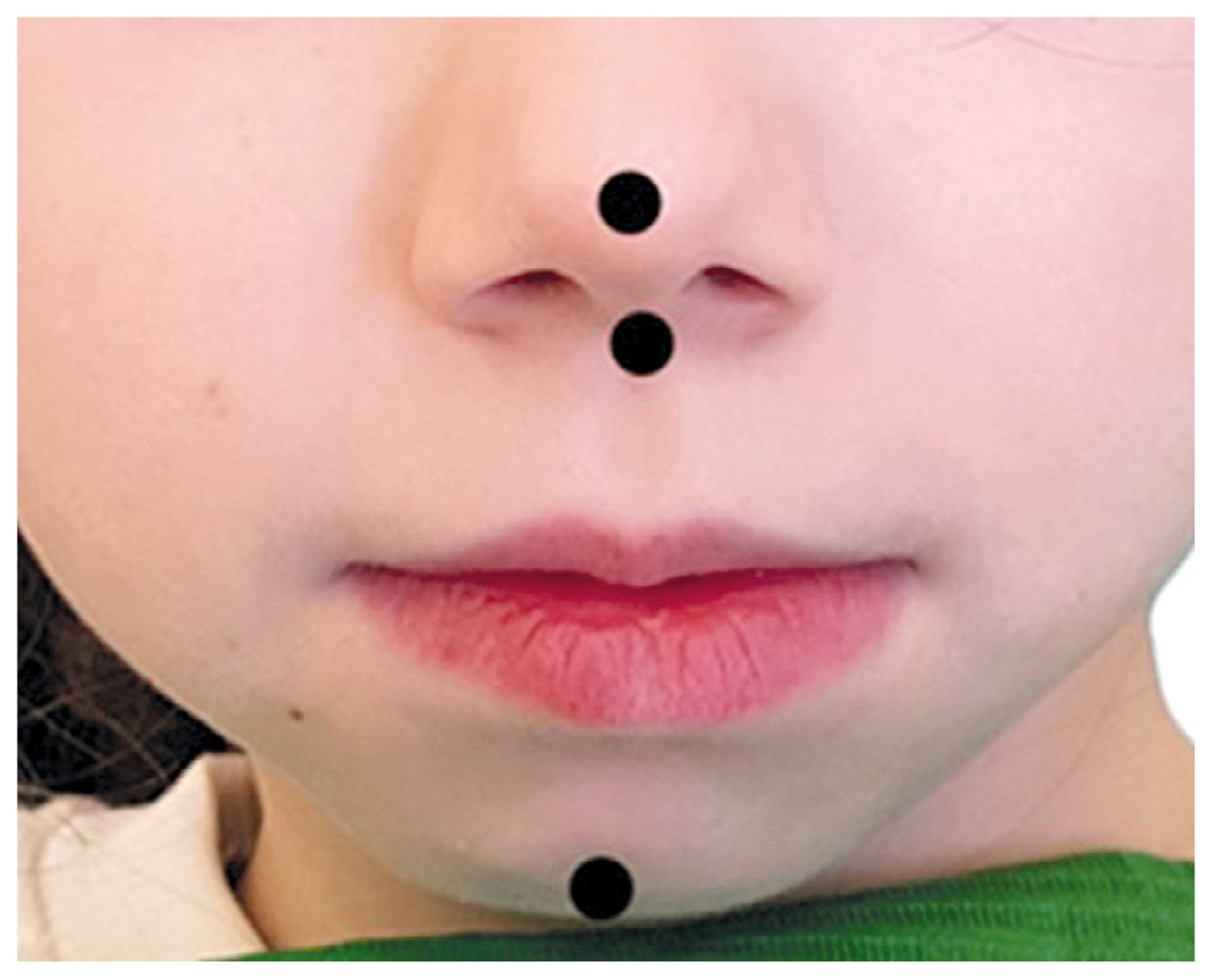
During the extraoral examination, visible facial asymmetry was noted, with the chin point (gnathion) deviating to the right both at rest and during movement. To objectively assess facial symmetry, an en-face photograph was taken, marked with anatomical landmarks: the trichion, ophryon, pronasale, subnasale, and gnathion. Ideally, these landmarks form a vertical midline that divides the face into symmetrical halves; however, in this patient, a noticeable deviation was present (Fig. 1). Palpation of the masticatory muscles and TMJ regions was conducted, revealing no tenderness or pain, and no joint sounds such as clicking or crepitus were detected during mandibular movement.
The MMO was assessed using a millimeter ruler to measure the distance between the incisal edges of the upper and lower central incisors (incision superius and incision inferius). This measurement was taken twice following standardized examination protocols [36]. The recorded MMO was 30 mm, which is considered reduced for children under 10 years of age (normal range: ≥ 35 mm) [5, 15, 37]. Mandibular deviation during mouth opening was also evaluated. In centric occlusion and at MMO, a pencil line was drawn on the lower central incisors, aligned with the midline between the upper central incisors. The distance between these lines indicated the degree of mandibular deviation in the frontal plane. A deviation of ≥ 2 mm was deemed pathological. In this case, a 5 mm deviation to the right was observed, exceeding the normal threshold (Fig. 2). Lateral excursions were assessed using a similar method. From the centric occlusion position, the patient was asked to perform maximal lateral movements to the left and right. Again, pencil lines were drawn on the lower incisors, extending from the midline of the upper central incisors. A lateral excursion range of ≥ 6 mm was considered normal. In this instance, movement was limited to 2 mm to the left and 7 mm to the right, indicating restricted mobility on the left side. Protrusive movement was measured by assessing the anterior translation of the mandible from centric occlusion. A millimeter ruler was used to determine the distance between the incisal edges of the upper and lower central incisors along the midline. A normal range was defined as ≥ 4 mm. The patient exhibited a limited protrusive movement of only 1 mm, suggesting restricted condylar translation.

A CBCT scan was performed to examine the bony structures. The morphometric analysis revealed:
right condyle: flattening and subcortical bone defects (score of 3 according to Billiau’s TMJ radiographic grading scale [20]);
left condyle: maintained morphology and cortical integrity (score of 0);
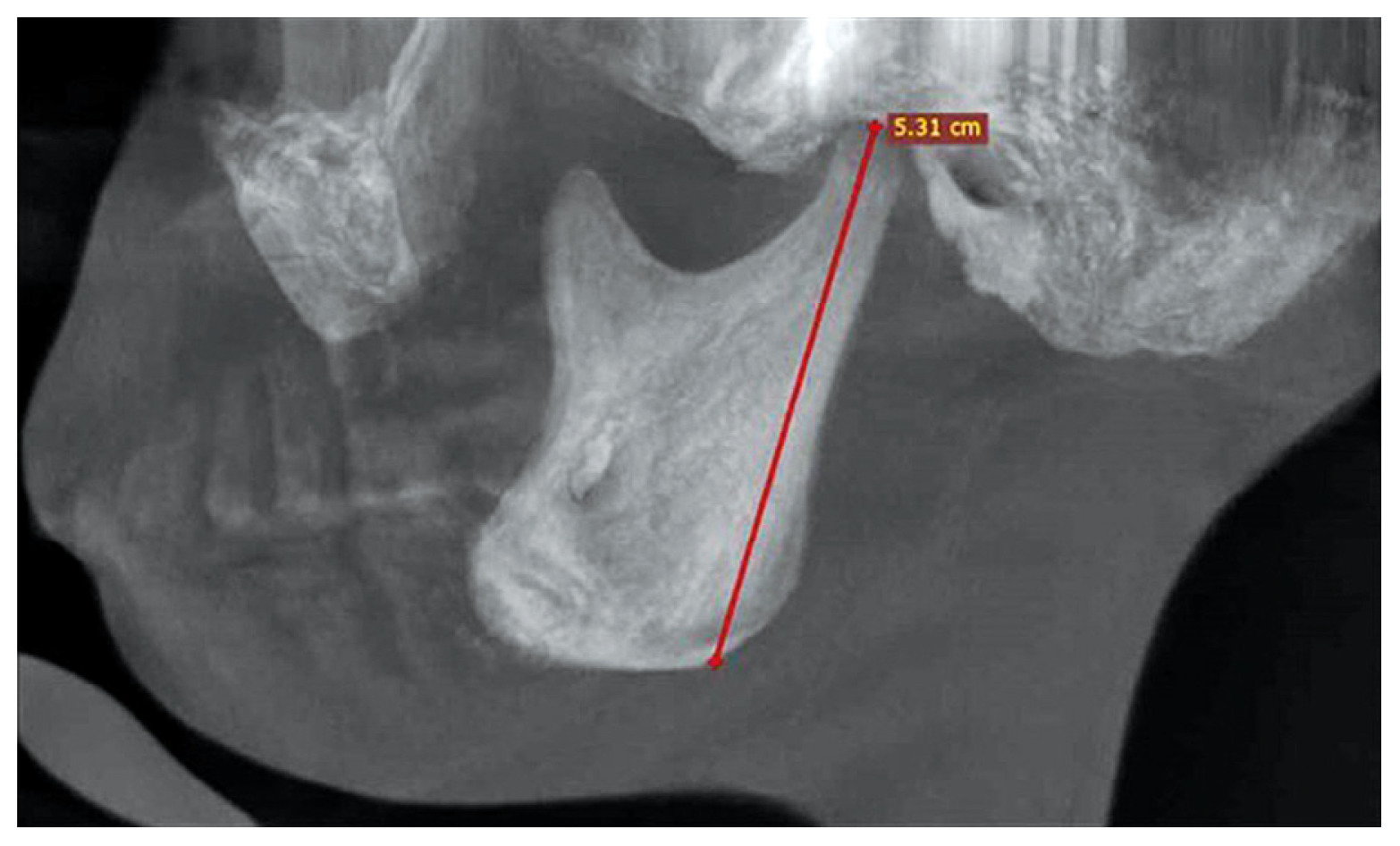
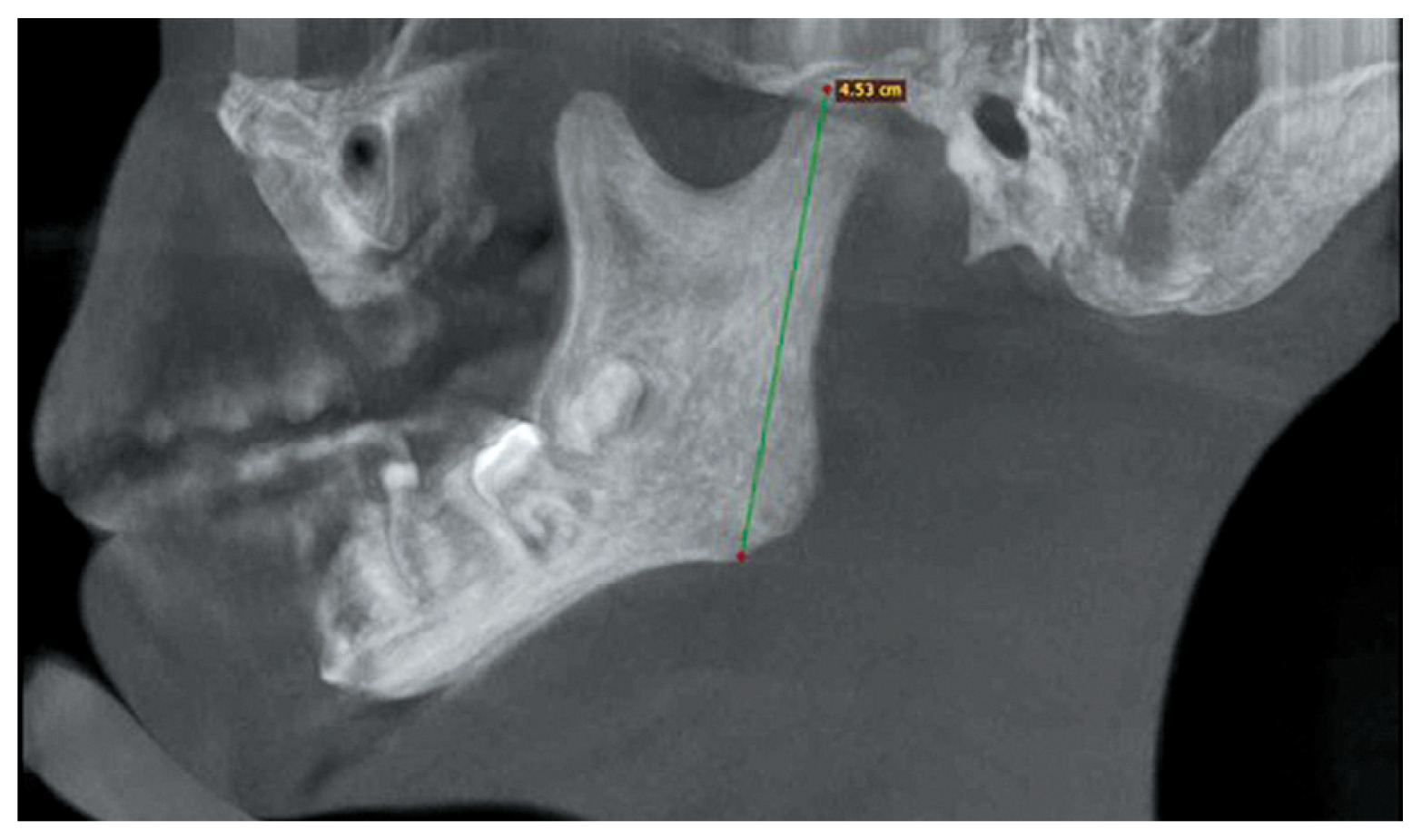
right mandibular ramus: reduced vertical height compared to the contralateral side, indicative of impaired growth likely caused by inflammation in the condylar center. The height of the mandibular ramus was measured from the condylion (the highest point on the condylar head) to the gonion, confirming asymmetry in ramus development (Figs. 3, 4).
Despite the absence of TMJ pain or subjective complaints, the combination of findings, facial asymmetry, restricted mouth opening and movement, and significant condylar remodeling observed on the CBCT, confirmed a diagnosis of unilateral TMJ arthritis. The overall clinical and radiographic findings were consistent with a diagnosis of unilateral TMJ arthritis, presenting in a silent, morphofunctional form without subjective symptoms.
Discussion
Temporomandibular joint arthritis in JIA poses a diagnostic challenge due to its often asymptomatic nature, particularly in early or unilateral cases. A case involving a 9-year-old girl with a 5-year history of polyarticular JIA illustrates this issue. This patient exhibited no TMJ-related symptoms but was found to have unilateral condylar disruption (on CBCT) and mandibular asymmetry, highlighting the concept of “silent” morpho-functional TMJ involvement. Although the child and her caregivers reported no TMJ-related complaints, including pain at rest, during chewing, or with jaw movement, and there was no history of trauma, orthodontic treatment, or masticatory dysfunction, the clinical examination revealed significant abnormalities. These included facial asymmetry, a reduced MMO, deviation of the mandible to the right, limited left lateral excursion, and protrusive movement. All these values fell below normative thresholds for her age.
An objective evaluation using standardized Clinical Orofacial Examination protocols and midline tracking confirmed asymmetrical jaw movement patterns. Crucially, CBCT imaging revealed flattening and subcortical bone defects of the right condyle, which were scored as 3 on Billiau’s TMJ radiographic grading scale. In contrast, the morphology on the contralateral side was preserved. Additionally, there was reduced height of the right mandibular ramus, measured from condylion to gonion, indicating impaired vertical mandibular growth likely due to condylar inflammation. The absence of joint sounds and pain upon palpation, together with this degree of morphological asymmetry and restricted movement, strongly suggests silent unilateral TMJ arthritis.
This case illustrates the concept of morphofunctional TMJ arthritis, where clinical asymmetry and functional limitations appear either before or in the absence of classic symptoms like pain or crepitus. Recent literature [15, 29] has reported similar cases in which radiographic changes in the condyle were observed in patients who did not present with any subjective complaints. These findings underscore the importance of conducting objective functional assessments and imaging protocols in the routine care of all children with JIA, even when they show no TMJ symptoms. Additionally, this case supports the notion that facial asymmetry and reduced jaw mobility should be considered primary clinical red flags for TMJ screening, especially when accompanied by risk factors such as a polyarticular disease course, a young age at onset, and a long disease duration. Researchers [15] emphasize the connection between disease duration and structural abnormalities in the TMJ, underscoring the progressive nature of untreated or subclinical joint involvement.
From a diagnostic perspective, the use of CBCT was crucial in confirming the presence of structural damage in the TMJ in this case. While MRI is considered the gold standard for assessing active inflammation, CBCT provides high-resolution images of bone structures and is particularly effective in detecting flattening, erosions, and condylar asymmetry – findings that are important for complex (pediatric dentist, orthodontic, and surgery) treatment planning. Although MRI was not performed in this case, which means active synovitis may have gone undetected, the severity of the remodeling observed on CBCT indicates a long-standing, likely inflammatory process. The unilateral shortening of the mandibular ramus indicates that TMJ arthritis has already impaired vertical growth on the affected side of the mandible. If left untreated, this asymmetry may worsen, potentially leading to permanent dentofacial deformities, such as micrognathia, anterior open bite, and functional occlusal disturbances. These issues extend beyond mechanical function and can affect aesthetic appearance, psychosocial well-being, and overall quality of life, particularly during adolescence – a time when social sensitivity is heightened.
This case emphasizes the clinical value of the Clinical Orofacial Examination protocol [18]. This protocol standardizes the assessment of jaw mobility, deviation, asymmetry, joint sounds, and tenderness. When systematically applied in rheumatology settings, such protocols can effectively bridge the gap between clinical observations and radiologic confirmations. The findings from this case illustrate how even a symptom-free patient can benefit from a structured morphofunctional evaluation, allowing for earlier detection and intervention.
The silent progression of TMJ arthritis necessitates proactive JIA diagnostic strategies. Key clinical insights from this case include the following: the absence of pain does not rule out significant TMJ pathology; facial asymmetry and restricted mandibular function are critical red flags, even in asymptomatic JIA children; CBCT can reveal advanced structural changes that may go unnoticed during a clinical examination; and standardized morphofunctional assessments, such as COFE, should be incorporated into routine follow-up visits for JIA. Early detection enables timely interdisciplinary interventions, which may help prevent long-term deformities.
This case-based review is limited by its focus on a single patient and the lack of MRI, which could have identified active inflammation. While the findings are illustrative, they may not apply to all subtypes or stages of JIA. Additionally, without long-term follow-up, we cannot assess the trajectory of disease progression or treatment response. Nevertheless, this case highlights a highly relevant and often underdiagnosed presentation of TMJ arthritis, underscoring its implications for clinical practice and screening policies.
Findings from larger studies support the importance of an individualized case perspective. Savioli et al. [13] demonstrated that 94% of JIA patients experienced TMJ dysfunction. Additionally, Mohamed et al. [28] reported that 35% of JIA patients exhibited TMJ-related symptoms, while 62% showed clinical signs, with reduced MMO being the most common sign, at 25%. Leksell et al. [14] observed reduced MMO in 32% of their cases, and similar findings were reported by Pawlaczyk-Kamieńska et al. [15] (58%). In contrast, Stoll et al. [12] and Koss et al. [21] found no significant differences in MMO between patients with TMJ arthritis and those without, highlighting a limitation in diagnostic specificity. Collin et al. [5] identified TMJ deformities in 39% of JIA patients using CBCT. These deformities were significantly associated with reduced MMO, pain upon palpation, and crepitus, which were often present even in asymptomatic individuals. Pawlaczyk-Kamieńska et al. [15] also reported facial asymmetry in 23% of patients and mandibular deviation in 46.15% of cases, with most deviations directed toward the more affected joint. Furthermore, their study showed that a younger age at onset correlated with greater lateral movement restriction toward the contralateral joint.
In summary, clinical examination alone lacks sufficient sensitivity and specificity in detecting TMJ involvement in JIA. Although features such as facial asymmetry, mandibular deviation, and restricted lateral movement may indicate TMJ pathology, a definitive diagnosis requires integration of clinical, functional, and radiographic data. Temporomandibular joint arthritis may lead to condylar growth inhibition and joint dysfunction, potentially resulting in progressive dentofacial deformity. However, when joint function and loading conditions are preserved, craniofacial development may proceed normally, even in the presence of structural abnormalities. These findings underscore the importance of early, comprehensive assessment and individualized monitoring in patients with JIA to prevent irreversible developmental complications.
Conclusions
This case highlights the importance of recognizing silent TMJ arthritis in JIA patients. The subtlety of symptoms can lead to delayed diagnoses and potential long-term implications, including compromised oral function and altered quality of life. Future research should focus on improving diagnostic methods and enhancing early detection strategies for TMJ involvement in children with JIA. Furthermore, longitudinal studies are essential to better understand the impact of silent TMJ arthritis on overall joint function and patient well-being, which can inform treatment protocols and improve outcomes in this vulnerable population.