
Introduction
The 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase (HMG-CoA) inhibitors, also known as statins, are a group of lipid-lowering medications that are used worldwide by approximately 25 million patients [1].
Statins are generally well tolerated and are very efficacious in treating high cholesterol levels through inhibition of 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase enzyme (HMGCR) controlling the metabolic pathway that produces cholesterol and other isoprenoids [2].
They are prescribed to reduce the risk of developing cardiovascular diseases and cerebrovascular diseases such as stroke or cerebrovascular accident [1].
Common side effects of statins include rhabdomyolysis, hepatotoxicity, diabetes mellitus, and myopathy [2]. Muscle-related side effects are the most common with the use of statins [1]. Normally, when a patient experiences myopathy, the medication is discontinued and the symptoms resolve [3].
Lately, however, there have been reports of cases with immune-related necrotizing myopathy with statin usage [3].
Statin-induced necrotizing autoimmune myopathy (SINAM) is very rare, with an incidence of 2–3 per 100,000 people [4]. This myopathy is characterized by significant progressive loss of muscle strength even after discontinuation of statin treatment [3, 4]. Autoimmune myopathies in general are acquired conditions that cause direct or indirect damage to muscle fibers through immune-related mechanisms [5].
The pathogenesis of SINAM is poorly understood, but there are several hypotheses; one suggests that statins cause over-expression of HMGCR in patients who are susceptible genetically through direct muscle toxicity resulting in necrotizing myopathy [6]. Another pathway describes a molecular modification of HMGCR that results in formation of anti-HMGCR antibodies, leading to an autoimmune response causing necrotizing myopathy [6].
It is crucial to diagnose SINAM promptly as early detection results in better treatment outcomes [1]. Along with symptoms of progressive proximal muscle weakness, laboratory testing is crucial in an attempt to identify this condition. Creatine kinase (CK) values have been known to go above 10 to 100 times the upper limit (2,000 and 20,000 IU/l) [7].
Electromyography may show features of myopathic lesions, with spontaneous fibrillations, positive sharp waves, myotonic or complex repetitive discharge and decreased duration of motor unit potentials [5]. Magnetic resonance imaging studies show T1 hypersensitivity with the short-T1 inversion recovery (STIR) signal being increased [5].
Normally, a biopsy of the muscles is taken as well, which, especially when the diagnosis is in doubt, may be conclusive. A typical biopsy for SINAM shows necrosis with the regeneration of muscle fibers with scarce inflammation that involves mainly macrophages [7]. Some other features of the condition include endothelial membrane attack complex deposition in the non-necrotic muscle fibers [7].
Statin-induced necrotizing autoimmune myopathy does have a genetic association. It has been proved that the human leukocyte antigen (HLA) DRB1*11 : 01 in adults and HLA DRB1*07 : 01 in children are significantly associated with myopathy with anti-HMGCR [7].
There have not been any reports of SINAM association with specific statins; however, atorvastatin and simvastatin have shown a higher correlation with SINAM than others [8]. In this article, we aim to analyze the clinical, serologic, and physiological characteristics of SINAM and determine the patients’ clinical characteristics, treatment and outcomes.
Material and methods
Data collection
The relevant literature was searched to identify articles for patients with SINAM. We searched the electronic databases PubMed, Google Scholar and Medline to identify published literature on this topic.
A detailed systematic literature search of the articles was performed until September 30th, 2021 using the following keywords, among others: “autoimmune”, “autoallergy”, “statin”, “HMG CoA reductase inhibitors”, “anticholesteremic agents”, “autoimmune myopathy”, “myositis”, “necrotizing myopathy”, “inflammatory myopathy”.
The inclusion criteria included case reports published between 2010 and 2021, as well as articles available in the English language. The exclusion criteria consisted of duplicate articles or abstracts only, animal studies, studies published before 2010, and articles published in languages other than English.
Demographic data
Age at onset, gender, weakness severity and distribution, and symptoms were extracted from the studies. Symptom duration was reported in months. Regarding weakness severity, if not explicitly stated in the article, we based our rating on the Medical Research Council grade of the weakest muscle group: 1 was rated as severe, 2 as moderate-severe, 3 as moderate, 4 as mild-moderate and 5 as mild. We assumed weakness distribution to be all proximal muscle groups unless otherwise stated.
Laboratory data
Creatinine kinase, troponin T, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), antinuclear antibodies, anti-Jo-1 antibody, signal recognition particle immunoglobulin G, 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase immunoglobulin G, and biopsy findings were extracted from the studies. In the case of several measurements of CK, the initial result on admission was recorded.
Treatment and outcomes
Treatment, time to reach remission, time to reach a low steroid dose, outcome and relapse data were also gathered. Treatment included steroids, either methylprednisolone or prednisone, intravenous immune globulin (IVIG), methotrexate (MTX), azathioprine (AZA) or a combination.
Statistical analysis
Descriptive statistics were used to summarize the patient characteristics of the collected case studies. Continuous data such as age, symptom duration and laboratory values are reported as mean with standard deviation.
Categorical data are reported as numbers with percentage. Crosstabulation was done using Microsoft Office Excel. Pearson’s χ2 test was used to analyze associations of categorical variables with a p-value of < 0.05 regarded as significant.
Results
Demographics and clinical features
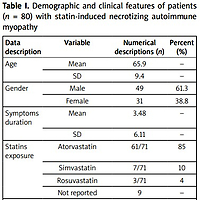
We identified 39 articles with a total of 80 patients meeting the study criteria for SINAM. Mean age of patients was 66 ±9.4 with the majority being male (61.3%) [9–46]. The mean duration of symptoms was 3.5 ±6.1 months.
All patients reported proximal muscle weakness and most patients reported moderate weakness involving both upper and lower extremities. Myalgia was found in 41% of analyzed patients and extra-muscular symptoms such as dysphagia (26.3%) and pulmonary complications such as dyspnea (5%) were also noted, as shown in Table I.
Table I
Demographic and clinical features of patients (n = 80) with statin-induced necrotizing autoimmune myopathy
Laboratory results
Our results showed a mean CK serum level of 10,094.2 ±7,351.7. The mean ESR from the cases where it was measured was 39.22 and the mean CRP was also elevated to 40.03 from the few cases where it was checked. Antinuclear antibodies were found only in two cases. Other myositis markers such as anti-Jo-1 and anti- signal recognition particle antibodies were negative in all of the studied cases. Anti-HMGCR was positive for 93.8% of patients. Only one patient had a negative test and one patient refused to undergo this test, and there were two cases with no report about test results.
The results of the tests are summarized in Table II. Most results from the muscle biopsy showed necrosis with minimal to no features of inflammation. Some of them showed regenerative muscle fibers.
Table II
Laboratory results
[i] Anti-Jo-1 – anti-histidyl transfer RNA synthetase, CK – creatine phosphokinase, CRP – C-reactive protein, ESR – erythrocyte sedimentation rate, HMGCR – 3-hydroxy-3-methylglutaryl-coenzyme A reductase, IgG – immunoglobulin G, SRP – anti-signal recognition particle, *n = 1 patient refused. The results are rounded to two decimal places.
Four patients refused therapy while the majority of patients (91.3%) were treated with glucocorticosteroids (GCs). The most commonly used GCs were methylprednisolone and prednisone (IV or oral); however, doses and treatment duration varied among cases. More than half (56.3%) of patients were also given intravenous immunoglobulins (IVIG). A summary of the treatment used is presented in Table III.
Table III
Summary of the treatment used
| Treatment | Time (months) | Number of patients (n) |
|---|---|---|
| No therapy | 4 | |
| GCs | 73 | |
| IVIG | 45 | |
| MTX | 30 | |
| AZA | 13 | |
| MMF | 7 | |
| Time to reach remission | 8.64 (mean) | |
| 9.10 (SD) | ||
| Time to reach low steroids | 4.39 (mean) | |
| 3.00 (SD) |
Time to reach remission was about 8.64 ±9.09 months. Approximately 42.5% returned to baseline while 10.0% did not see any improvement. There was a 3.8% mortality rate even after treatment and in 10.0% of cases the symptoms recurred. The outcome summary is presented in Table IV.
Table IV
Outcome of the disease
| Outcome | Number of patients (n) | Percent of patients (%) |
|---|---|---|
| Return to baseline | 34 | 42.5 |
| Symptom improvement | 26 | 32.5 |
| No improvement | 8 | 10 |
| Mortality | 3 | 3.8 |
| Not associated | 9 | 11.3 |
| In total | 80 | 100 |
| Relapse | 8 | 10 |
Crosstabulation analysis was done to identify any relationship between age, gender and weakness severity, and the type of therapy with patient outcome. We stratified age groups from 40 to 90 years old in increments of ten. No significant difference in weakness severity was observed according to gender (p = 0.87) or age (p = 0.49).
Treatment groups were identified as follows: (1) No therapy, (2) GCs alone, (3) GCs + disease-modifying anti- rheumatic drug (DMARD), (4) GCs + IVIG and (5) GC + IVIG + DMARD. Disease-modifying antirheumatic drugs were either MTX or AZA or a combination of both.
50% of cases in the no therapy group returned to baseline while 50% saw no improvement. Patients treated with only GCs had a 35% return to baseline, 25% improvement of symptoms, 10% no improvement, and 5% mortality was demonstrated.
Patients treated only with GCs had a 35% return to baseline, 25% had symptoms improvement, 10% reported no improvement, and 5% mortality was described. In the group treated with GCs + DMARD, 27.27% of patients returned to baseline while 45.45% of patients had symptoms improvement.
In the group treated with GCs + IVIG, 50% of patients returned to baseline, 14.29% had improvement of symptoms, and 14.29% had no improvement. In this group 14.29% mortality was noted.
We observed that a significant number of patients treated with a combination of GCs + IVIG + DMARD either returned to baseline or had improvement in their symptoms (92.86%) as compared to other treatment regimens (p = 0.02).
Discussion
Statins are the first-line treatment for hyperlipidemia, used in the primary and secondary prevention of atherosclerotic cardiovascular disease (coronary artery disease or stroke) [47].
Immune-mediated necrotizing myopathy (IMNM) is an autoimmune myopathy characterized by severe proximal muscle weakness. There is minimal inflammatory cell infiltration leading to myofiber necrosis which is seen on muscle biopsy. Thus far, two varying autoantibodies are associated with IMNM, those targeting the signal recognition particle and those targeting HMGCR [48].
Statins are usually well tolerated. However, statin- associated muscle symptoms are the most common side effects, which can range from myalgias without any spike in CK serum levels to myalgias with a significant increase in CK concentration.
Up to 20% of patients with SINAM have mild symptoms such as myalgias which may occur and get better after discontinuation of such treatment [5]. However, in a small percentage of patients despite discontinuation of the statins, symptoms and laboratory findings persist.
Needham et al. [49] first presented a case series of patients where they described eight patients developing autoimmune myopathy in the context of statin use and it persisted even after discontinuation of the medications [5, 49].
Christopher-Stine et al. [50] then first described the association of the antibody with IMNM frequently associated with previous statin use and named it as anti-200/100 antibody.
Mammen [51] later recognized it as an anti-HMG-CoA reductase antibody. Statin-induced autoimmune myopa-thy needs treatment with GCs or IVIG or disease-modifying agents alone or in combination to stop the disease process.
Demographic variables
In the analyzed cases we noted a wide age range of the patients, from 46 to 86 years. Our review identified mostly older patients (65.9 + 9.4), which was similar to other reviews published on statin-associated autoimmune myopathy [3]. Male predominance (61.3%) was observed in the analyzed patients, which was high compared with previously published studies [3].
Clinical presentation
Patients had an average disease duration of 3.5 months before they presented to the hospital, which is similar to the previously presented data [49]. With the exception of a few patients, almost all of them had muscle weakness ranging from mild to severe, affecting their daily activities.
The bilateral proximal extremities were mostly affected.
Myalgia and dysphagia were other commonly presenting symptoms. Weight loss and even skin involvement were found in some patients.
Laboratory investigations
The creatine kinase serum levels were invariably raised in all cases, on average 67 times higher than the normal upper limit of 150 IU/l. It is higher than the CK levels noted in the Nazir et al. [3] study. Anti-HMGCR ELISA testing has 99% specificity and 94% sensitivity for diagnosing anti-HMGCR antibodies [5].
The gold-standard test for diagnosing statin-associated auto-immune myopathy anti-HMGCR antibody was positive in all but one patient. Similar results have been observed in previously published data.
In the Mammen [51] study, it was noted that anti- HMGCR autoantibodies found in younger patients presenting with autoimmune myopathy without prior statin use were less responsive to therapy.
A study by Mohassel et al. [5] noted that anti-HMGCR antibody-positive autoimmune myopathy is rarely seen in the case of other connective tissue diseases such as systemic scleroderma and interstitial lung disease. These cases also had positivity for other autoantibodies (anti-PM-Scl and anti-Jo-1 antibodies) and no prior statin use in the medical history [5].
Needham et al. [49] also described a case with a weakly positive anti-Jo-1 antibody but it was inconsistent in other SINAM cases. All of the patients in this study had prior statin use history, and other antibodies were mostly negative. The most prominent histologic feature in statin-associated autoimmune myopathy was muscle-cell necrosis and regeneration [51].
Except for a few cases, all muscle biopsy results show necrosis with minimal or no inflammation, whereas 25.32% of the biopsies showed regeneration. We also observed some cellular infiltrates, mainly macrophages and very few T cell lymphocytes. These histologic features support our diagnosis of autoimmune myopathy. Our pooled data do not show major histocompatibility complex class I molecules in muscle biopsy, which is different from Mammen [51].
Treatment and outcomes
Immunosuppressants and statin cessation were the primary treatment modality [3]. We noted that almost all patients needed immunosuppressant therapy, alone or in combination, to recover. Only two patients returned to baseline without any treatment. 32.5% of cases never fully returned to baseline, and 3.75% of cases resulted in mortality even after treatment. Nazir et al. [3] reported that 83.82% of the SINAM patients required two or more immunosuppressants, whereas our analysis revealed a lower percentage (53%) of patients who required two or more immunosuppressants [3].
Study limitation
The results of this systematic review were derived based on case reports and case series. Inclusion criteria also limited the review to English literature on the various databases that were searched. Therefore, due to limited extensive research and data on the subject, clinical trial data were scarcely used.
Conclusions
The majority of patients treated with statins tolerate these drugs without any adverse effects. However, few patients may develop symptoms of myositis and in laboratory assessment elevated CK serum levels.
Persistence of proximal muscle weakness, myalgias, and elevated CK levels, two times or higher than the upper limit even after discontinuation of statins should be a stimulus to physicians to diagnose SINAM. Early physical examination and assessment of these patients with laboratory, antibody testing, and muscle biopsy help confirm the diagnosis.
The authors recommend prompt cessation of statins and initiation of immunosuppressants to reduce morbidity and mortality in this group of patients. We also advocate further research to ascertain whether these patients, once improved, may benefit from re-challenging with statins.