
Introduction
Ankylosing spondylitis (AS) is one of the pressing problems of modern rheumatology and is often associated with severe somatic disorders, decreased self-care ability, a deterioration of the quality of life, and a reduction of life expectancy of patients [1, 2]. The main AS manifestation is chronic pain, the persistence of which in some cases is caused not only by inflammation, but also by the presence of neuropathic pain (NP) [3–5]. The impact of NP on AS patients is very significant, as it greatly complicates the patients’ everyday activities and leads to a decrease of the life quality [6–8].
At the same time, diagnosing NP is a challenging complex task that has not yet been fully resolved, which causes the researchers to continue searching for effective diagnostic techniques, including those aimed at differentiating pain syndromes of various genesis [9–11]. Late NP diagnostics lacking appropriate therapy reduce the treatment efficacy for this category of patients [12]. Neuropathic pain should be established by appropriate screening tools, such as: questionnaire: Neuropathic Pain 4 (Douleur Neuropathique en 4 Questions – DN4) and Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) [13]. Other diagnostic methods are also important [14].
Taking this into account, it is important to keep improving diagnostic and therapeutic approaches for assessment of NP prevalence and activity/severity using various rating tools.
The objective of the study was to analyze prevalence of NP in patients with AS and clinical features of AS patients depending on the presence of NP.
Material and methods
We examined 142 patients who were hospitalized at the Center of Rheumatology, Osteoporosis and Biological Therapy of the communal non-profit enterprise “Vinnytsya Regional Clinical Hospital named after M.I. Pirogov” between December 2019 to October 2022. Diagnosis of AS was established according to modified New York criteria [15].
The patients were divided into two groups: the first group of 94 patients with AS without NP, and the second group of 48 AS patients with NP. The mean age of all patients was 41.9 ±9.7 years; patients with NP were slightly older: 44.0 ±8.4 years vs. 40.9 ±10.2 years (p = 0.063). The period from the onset of disease (first complaints) to the diagnosis of AS in all patients was 6.0 ±4.6 years; in patients with NP it was slightly longer: 6.4 ±4.7 years vs. 5.7 ±4.5 years (p = 0.403). The duration of AS from the appearance of the first symptoms to the inclusion in our study in all examined patients was 9.6 ±6.4 years; the duration of the disease in patients with NP was slightly longer: 10.3 ±6.4 years vs. 9.3 ±6.5 years (p = 0.273).
The average body weight in all patients was 77.6 ±10.6 kg, in patients with NP it was 74.8 ±12.5 kg vs. 79.0 ±9.3 kg (p = 0.091) in patients without NP, body mass index was 25.9 ±3.58 and 26.08 ±2.56, respectively (p = 0.900). All patients received standard treatment for AS before the examination.
Patients with mental disorders, and severe somatic diseases were excluded from this study.
The NP was revealed by the LANSS [16] and the DN4 [17]. Once a subject had a positive result on both tools (12 or more LANSS points, and 4 or more DN4 points), the patient was assigned to the NP group.
The Standardized Evaluation of Pain (StEP) was used to assess the NP severity [18]. The Bath AS Functional Index (BASFI) [19] and Bath Ankylosing Spondylitis Metrology Index (BASMI) [20, 21] were used to assess functional ability in AS patients. The disease activity was assessed by the Bath Ankylosing Spondylitis Disease Assessment Index (BASDAI) [22] and Ankylosing Spondylitis Disease Activity Score (ASDAS) [23] tools.
The general state of health and functions of AS patients were assessed according to the Health Assessment Questionnaire (HAQ) [24].The Ukrainian-language adapted version of the ASAS Health Index and Environmental Factors (ASAS HI/EF) questionnaire [25] and the Bath Ankylosing Spondylitis Patient Global Score (BAS-G) were used to assess the patients’ state of health [26].
The differences were statistically evaluated using Fisher’s and Mann-Whitney non-parametric tests. Correlational analysis was performed using the Spearman rank order correlations method.
Results and discussion
The overall prevalence of NP regarding LANSS in AS patients was 36.6%, 51.7% in females vs. 32.7% in males (p = 0.048); while according to DN4 prevalence of NP was 38.0%, 58.6% in females vs. 32.7% in males, (p = 0.010). In both tools, NP was found in 33.8% of AS patients, significantly more often in females than in males: 51.7% vs. 29.2%, respectively (p = 0.021).
Clinical characteristics of patients with AS according to presence of NP are presented in Table I.
Table I
Characteristics of patients with and without neuropathic pain according to various diagnostic scales (points)
[i] ASAS HI and EF – Ankylosing Spondylitis Activity Score Health Index and Environmental Factors, ASDAS – Ankylosing Spondylitis Disease Activity Score, BAS-G – Bath Ankylosing Spondylitis Global score, BASDAI – Bath AS Disease Activity Index, BASFI – Bath AS Functional Index, BASMI – Bath Ankylosing Spondylitis Metrology Index, DN4 – Douleur Neuropathique 4 Questions, HAQ – Health Assessment Questionnaire, LANSS – Leeds Assessment of Neuropathic Symptoms and Signs, M – mean, Me – median, Non-NP patients – patients without neuropathic pain, NP patients – patients with neuropathic pain, p – statistical significance of differences, Q25–Q75 – interquartile range, SD – standard deviation, StEP – Standardized Evaluation of Pain.
The analysis of NP in AS patients made it possible to reveal rather high severity rates of NP. The patients assigned to the NP group presented the expectedly high scoring according to LANSS compared to the non-NP group of patients, which suggested the presence of certain elements of the NP syndrome, that did not reach the rate of clinical expressiveness. The DN4 questionnaire findings presented similar patterns, which was consistent with the LANSS assessment data.
The StEP questionnaire made it possible to effectively differentiate neuropathic and nociceptive pain. All NP patients regarding StEP scored 4 or more points, which differentiated neuropathic and nociceptive pain, while non-NP patients presented less than 4 points. The obtained data suggested that the AS population was characterized by generally elevated NP expressiveness rates, mainly on account of patients with clinically shaped NP; however, patients without NP also presented some NP manifestations, which, nevertheless, did not reach the clinical expression rate.
The BASDAI in NP patients appeared to be statistically significantly higher than in non-NP subjects. The analysis of the BASDAI distribution of all AS patients showed that most patients belong to the high activity group. At the same time, only one NP patient belonged to a low activity group and other subjects fell into the high activity group, while in the non-NP group, high and low activity was established in the majority and minority of patients, respectively (Table II).
Table II
Clinical features of patients with and without neuropathic pain
[i] AS – ankylosing spondylitis, ASDAS – Ankylosing Spondylitis Disease Activity Score, BASDAI – Bath AS Disease Activity Index, BASFI – Bath Ankylosing Spondylitis Functional Index, BASMI – Bath Ankylosing Spondylitis Metrology Index, HLA – Human Leukocyte Antigen, Non-NP patients – patients without neuropathic pain, NP patients – patients with neuropathic pain.
The HLA-B27 test, the main immunogenetic marker of susceptibility to AS, showed positive results somewhat more often in patients with NP – 75.0% vs. 70.2% in patients without NP; however, these differences were statistically insignificant (p > 0.05) (Table II).
Similar data were obtained by analyzing the activity according to ASDAS. The moderate ASDAS score was significantly higher in NP patients. The analysis of ASDAS distribution revealed the same pattern as for BASDAI (Table II).
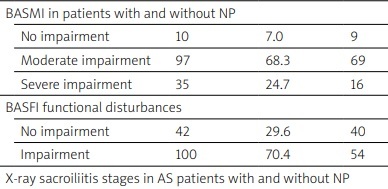
The evaluation of functional ability depending on NP showed that NP established a number of regularities. According to BASMI physical dysfunction in patients with NP was significantly higher compared to patients without NP. All patients with AS according to BASMI were divided into three groups: no functional impairment, moderate impairment, and severe impairment; first group had the fewest patients, the second group had more than two-thirds, and the third group had about a quarter. At the same time, the NP patients presented a significantly higher percentage of patients with pronounced functional impairment, while non-NP patients had a higher percentage of patients with moderate impairment (Table II).
The BASFI analysis provided similar data. The assessment of patient group distribution depending on the presence or absence of functional impairment revealed impairment in the majority of AS patients. At the same time, functional impairment were established in almost all NP patients, and in more than half of non-NP patients (Table II).
Health assessment by the ASAS HI/EF showed that patients with NP had no significant difference compared to patients without NP. On the other hand, self-reported BAS-G symptoms in the first week (BAS-G 7 days) and during the last 6 months (BAS-G 6 months), as well as in general (BAS-G Score), showed a significantly worse index of health in patients with NP compared to patients without NP.
Patients with NP also had a significantly higher HAQ, indicating an association of NP with poorer health and reduced functional capacity.
The study of the radiological features of AS in NP and non-NP subjects did not reveal any significant difference (Table II).
The HLA-B27 test, the main immunogenetic marker of AS susceptibility, presented somewhat more frequent positive results in NP patients (Table II).
Correlation analysis between various indicators of activity and functional ability in AS showed the presence of a significant direct correlation of mostly moderate (rank correlation coefficient values from 0.3 to 0.7) and weak (rank correlation coefficient values up to 0.3) strength: BASDAI and ASDAS (r = 0.656); BASDAI and BASMI (r = 0.327); BASDAI and BASFI (r = 0.543); ASDAS and BASMI (r = 0.267); ASDAS and BASFI (r = 0.411); BASMI and BASFI (r = 0.541). Significance of differences between groups was at the level of p < 0.01.
Correlational analysis revealed that LANSS value significantly correlated with disease activity and functional ability: BASDAI (r = 0.501; p < 0.01), ASDAS (r = 0.374; p < 0.01), BASMI (r = 0.235; p < 0.01), BASFI (r = 0.574; p < 0.01). The DN4 also showed a significant correlation with BASDAI (r = 0.506; p < 0.01), ASDAS (r = 0.357; p < 0.01), BASMI (r = 0.249; p < 0.01), BASFI (r = 0.465; p < 0.01). The closest relationship was found between markers of NP and the BASFI (functional disability) and the BASDAI (disease activity), less closely – with the ASDAS and BASMI.
The obtained results indicate the presence of specific differences in the activity of the disease, the severity of functional disorders, and the well-being of patients with AS depending on the presence of NP. Patients with NP have significantly higher disease activity, significantly greater disability, and poorer general health. These findings should be taken into account when developing an individual approach to treatment.
Conclusions
Ankylosing spondylitis is associated with significant prevalence of NP, established in about a third of male and more than half of female patients. Neuropathic pain is associated with significantly higher disease activity, greater loss of functional capacity, and decreased general health status. It allows NP to be considered as an aggravating factor for these manifestations. At the same time, no significant differences were found in the severity of NP in patients with different radiological grades and HLA-B27 positivity.
Indicators of activity and functional ability in AS are related to each other, as well as to indicators of the severity of NP by a direct correlation of a moderate and weak degree.
The obtained data might be useful for understanding the pathogenetic mechanisms of NP in AS patients.They should be taken into account when developing treatment approaches for these patients.
Prospects for further research are related to a comprehensive study of the interaction of various aspects in patients with AS, taking into account the NP. Improving approaches to treatment and rehabilitation of these patients should also take into account the presence of NP.