
Introduction
The major cause of physical disability in the world is musculoskeletal diseases. The World Health Organization (WHO) in 2011 presented the World Report on Disability and according to this report in the adult population (> 18 years) the average rate of disability was 15.6%, but there are differences between high and low income countries (from 11.8% to 18% respectively) [1]. Disability was reported more often in the elderly group (over 60), as well as in women and in the poorest group.
Among the people with issued disability certificates there is also a population of children with different diseases. Disability assessment systems for both children and adults are being developed in various countries.
The Polish disability certification system is characterized by a significant level of complexity. At the same time, there are separate regulations for pension purposes: the Social Insurance Institution (ZUS), Agricultural Social Insurance Fund (KRUS) and pension systems of uniformed services. A separate structure is the system for issuing disability certificates: poviat/city disability adjudication teams, voivodeship disability adjudication teams, the Ministry of Family and Social Policy supervising poviat and voivodeship teams. The system is complemented by the appeals to the court which resolve complaints against the decisions of voivodship teams [2].
Issuing certificates on children’s disability is carried out by poviat/city disability adjudication teams, supervised in the second instance by voivodeship teams. However, “children” are understood as persons up to 16 years of age, and persons over 16 years of age are considered “adults”. This division is a formal one. The basic difference in issuing disability certificates for individuals up to 16 years of age is that they are given disability certificates without grading and for people over 16 years of age, disability is graded by distinguishing mild, moderate and severe disability.
The aim of this article was to investigate the characteristics of children obtaining a disability certificate due to diseases of the locomotor system within the last 16 years.
Material and methods
The authors asked the Municipal Disability Adjudication Council in Lublin to provide data on the number of disability certificates issued for children up to 16 years of age in the years 2006–2021.
The rules of recognition of a person under 16 as disabled requires that the following criteria be met:
impairment of the physical or mental fitness of the body, where the estimated duration of the condition is over 12 months,
impairment of the body’s efficiency caused by a congenital defect, long-term disease or damage,
impairment of the body’s efficiency resulting in the need to provide complete care or assistance in meeting basic life needs, and this is to be done in a way that exceeds the support needed by people of a given age [3].
The further development and specification of the criteria, disease states and the rules for assessing the child’s condition have been included in the provisions of the ordinance.
When assessing children’s disability, the following criteria are taken into account:
whether there is a projected duration of disability due to medical conditions exceeding 12 months,
is there an inability to meet basic life needs, such as: self-service, independent movement, communication with the environment, necessitating the provision of constant care or assistance, in a way that exceeds the scope of care for a healthy child at a given age,
whether there are significant disturbances in the functioning of the body, requiring systematic and frequent medical and rehabilitation treatments at home and outside the home.
The regulations specify a catalogue of diseases that justify the need for permanent care or assistance to a disabled person up to 16 years of age. These are:
congenital anomalies and diseases of various aetiology leading to paresis, paralysis of limbs or changes in the musculoskeletal system, significantly impairing the grasping ability of the hands or hindering independent movement,
congenital or acquired severe metabolic diseases, cardiovascular, respiratory, urinary, digestive, coagulation and other diseases significantly impairing the body’s efficiency, requiring systematic treatment at home and periodic hospital treatment,
mental retardation ranging from moderate to severe,
psychoses and psychotic syndromes,
pervasive developmental disorders causing significant disturbances in activity, social interactions or verbal communication, interests and activity,
epilepsy with frequent seizures or clear psychoneurological sequelae,
malignant tumours and proliferative diseases of the haematopoietic system up to 5 years after the end of treatment,
congenital or acquired defects of the organ of vision causing a significant limitation of its efficiency, leading to a decrease in visual acuity in the better eye to 5/25 or 0.2 according to Snellen after correcting the vision defect with corrective lenses, or limiting the field of vision to the space within 30 degrees,
deafness or a double-sided hearing impairment not improving sufficiently with a hearing aid or cochlear implant [4].
As in the case of adults, the criteria for determining children’s disability were formulated based on the health condition and diagnosed deficits of the disabled person, and not on the possibilities and aspirations of an individual. A further weakness of the Polish system of adjudication is its detachment from the assessment of a person’s living environment and the impact that the environment has on the level of their functioning. This is the cause of a lot of controversy over the manner of certifying disability in children and adults.
A different description of disability is contained in the International Classification of Functioning, Disability and Health (ICF) by the World Health Organization (WHO), which takes into account both a person’s characteristics and personal situation and the influence of the surrounding environment [5, 6].
Results
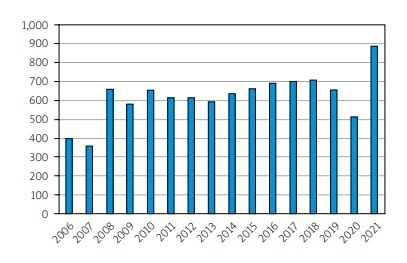
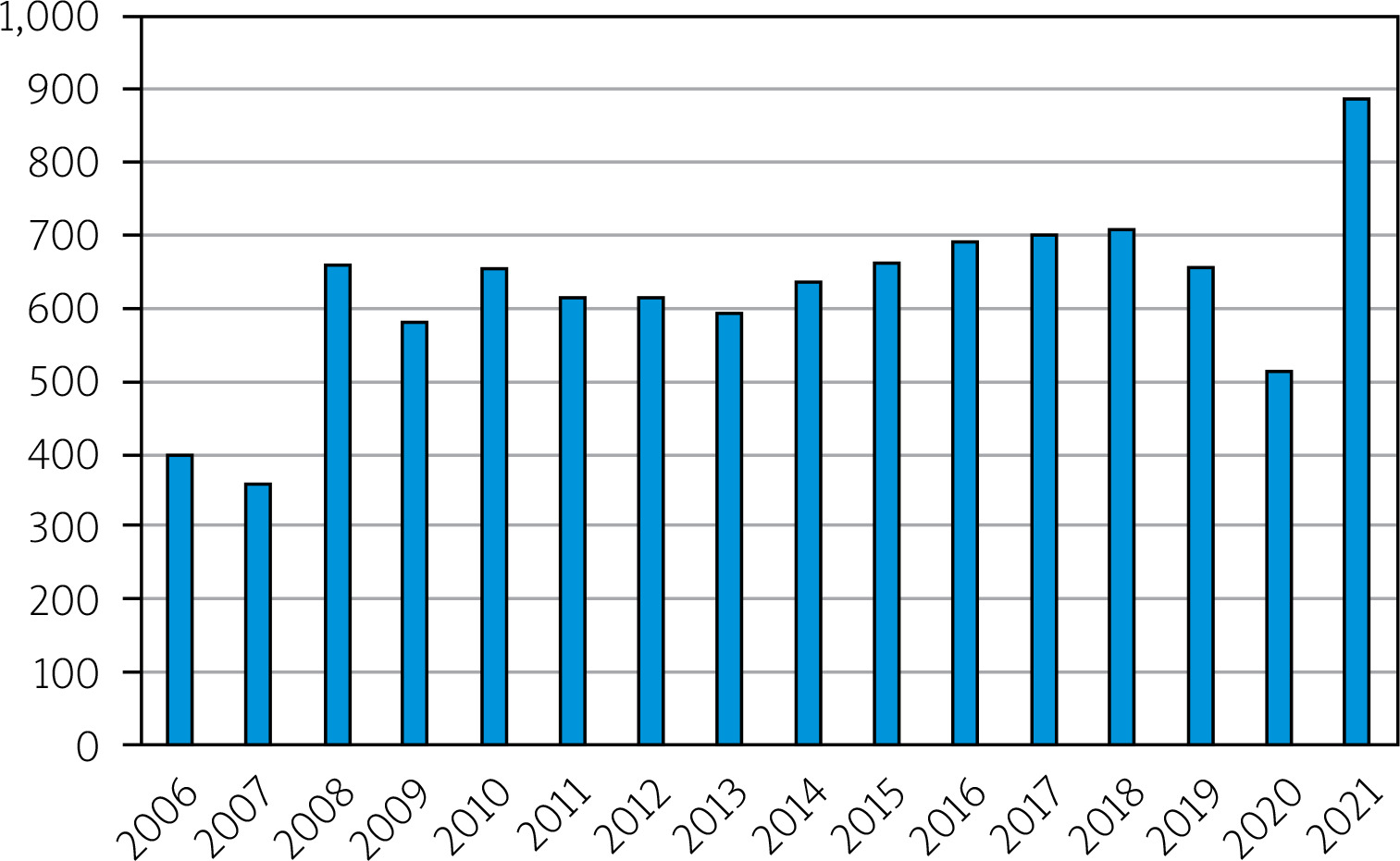
Data from the Municipal Disability Adjudication Council in Lublin were collected from the years 2006–2021. In this period 9,929 disability certificates for children up to 16 years of age were issued. The mean number of issued certificates was 620 per year (Fig. 1).
Fig. 1
Number of disability certificates issued by Municipal Disability Adjudication Council in Lublin for children 0–16 years of age in the years 2006–2021.
The numbers of certificates issued for children in Lublin are shown in Figure 2.
Fig. 2
Health problems being the reason for obtaining disability certificate in < 16 group in Lublin in the years 2006–2021.
The reasons for obtaining disability certificates are symbolized with the following letters:
C – developmental disorders before the age of 16, E – epilepsy, I – other diseases including endocrine diseases, metabolic diseases, enzymatic disorders, infectious and zoonotic diseases, deformities, diseases of the hematopoietic system, L – disorders of voice, speech and hearing disorders, M – diseases of the genitourinary system, N – neurological diseases, O – eye diseases, P – mental illness, R – diseases of the musculoskeletal system, S – diseases of the respiratory tract, T – diseases of the digestive system, U – mental retardation.
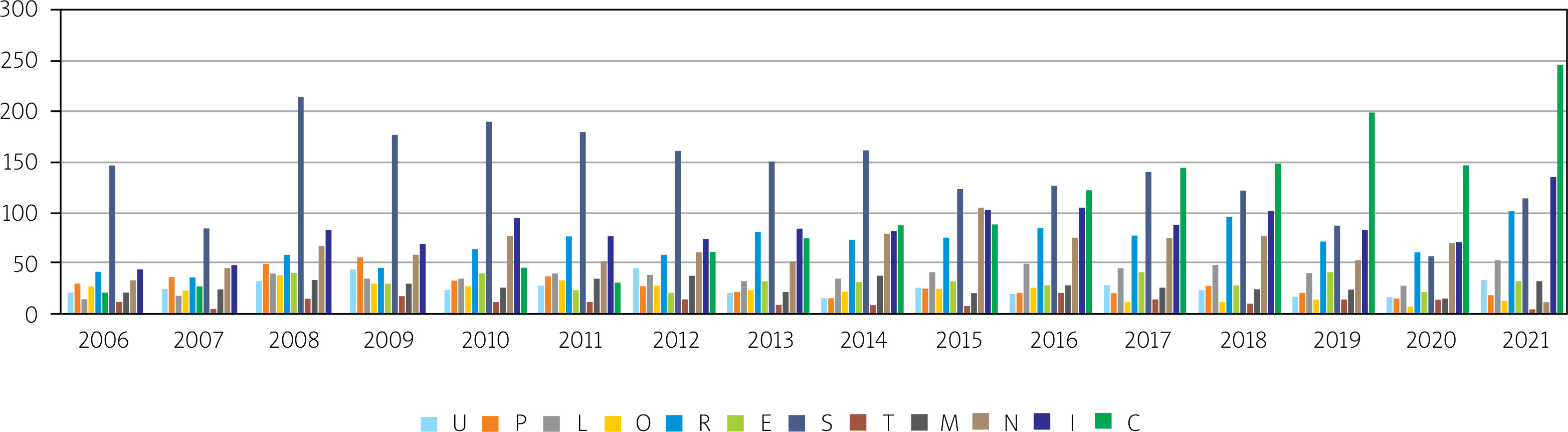
Diseases of the respiratory tract are the leading (22%) cause of obtaining a disability certificate in the under 16 group. Developmental disorders are in the second position (13%) and musculoskeletal diseases are the reason for issuing 11% of such certificates.
The total number of certificates issued because of musculoskeletal disorders was 1,085 (mean 68/year). The majority of them were given to children 8–16 years old (Fig. 3).
Fig. 3
The age of children with disability certificated due to the diseases of the musculoskeletal system.
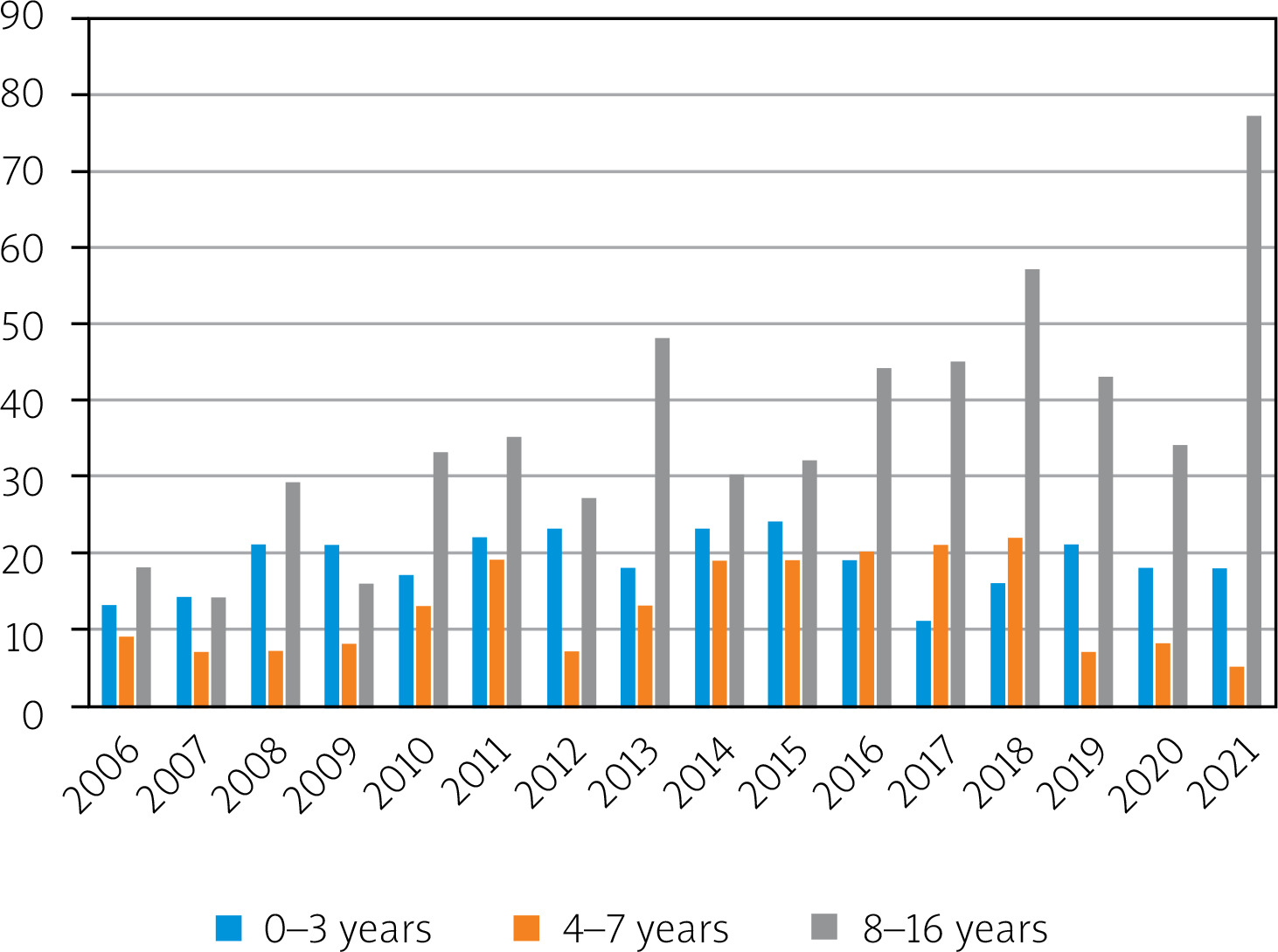
Within the years 2006–2021 524 girls (mean 32.75/year) and 561 boys (mean 35.06/year) received the disability certificate due to diseases of the musculoskeletal system.
Discussion
According to UNICEF there are nearly 240 million children living with disabilities worldwide – 1 in 10 of all children. Among children aged 2–4 years, 38% of them live with more than one functional difficulty. In South Asia there are 64.4 million children aged 0 to 17 with disabilities, in West and Central Africa 41.1 million, in Eastern and Southern Africa 28.9 million, in East Asia and the Pacific 43.1 million, in the Middle East and North Africa 20.3 million, in Latin America and the Caribbean 19.1 million, in Europe and Central Asia 10.8 million and in North America 8 million [7, 8].
According to the data of the Statistics Poland (Główny Urząd Statystyczny – GUS) in Poland, for the needs of educating people with disabilities and people with special educational needs, in the school year 2020/2021 there were 318 special kindergartens attended by 6,000 children, while 46,800 attended special primary schools [9].
The Statistics Poland reports the highest number of people with a certificate of disability or unable to work because of disability in Poland per 10,000 of the population in the Lubuskie Voivodship (890). The indicator exceeded 700 people in the following voivodeships: Wielkopolskie (723), Świętokrzyskie (721), Podkarpackie (712), Kujawsko-Pomorskie (708) and Warmińsko-Mazurskie (706) [9]. But the above data are collected for adults not for children. The disability assessment system in Poland is not uniform and a reform of the disability assessment system is being conducted [10].
Statistical research on self-assessment of health is conducted among people aged 16 and over. Statistical offices in Poland and in the world do not conduct such surveys with the participation of children. Only UNICEF does.
In Europe, the EU Statistics on Income and Living Conditions (EU-SILC) survey has been conducted since 2004, under the supervision of the European Statistical Office (EUROSTAT), in which respondents aged 16 and over are asked the question “How do you rate your health overall?”. In Poland, this study is conducted by the Statistics Poland on a sample of residents of 24,000 randomly selected apartments in the country. Based on it, we learn that 17% of men and 14.1% of women in Poland assess their health as good. On the other hand, 48.9% of men and 44.6% of women residents of Greece do so, 48.4% of men and 45.3% of women in Cyprus and 45.7% of men and 43.3% of women in Ireland [11].
With age, self-assessment of health is worse and worse. In the European Union among people aged 16–24, 90% of men and women (both in the EU on average and in Poland) assess their health as good or very good. On the other hand, at the age of 55–64, only 42% of Poles and Polish women evaluate their health in this way, while the average for Europe is 60% [12]. The Gallup Institute in the US, commissioned by the United Nations (UN), studies the happiness index. Poland is there in the 41st position. For several years, Denmark has been in first place, although in terms of average life expectancy, Denmark is in 23rd place, and Poland in 40th [13].
The number of disability certificates issued by the Municipal Disability Adjudication Council in Lublin for children is much lower than for adults. In the years 2006–2021 it issued 76,581 certificates for people > 16 years of age (mean 4,786 certificates per year) [14]. As we have found for children it was 9,929 (mean 620/year). Of course, one of the reasons for this disproportion is the fact that childhood in the aspect of disability certification lasts from 0 to 16 years of age.
The proportion of musculoskeletal system disorders to other health problems as the basis for issuing disability certificate significantly differs in the adult group vs. children. In the adult group locomotor problems are the leading cause of issuing disability certificates while in children they are in the third position after diseases of the respiratory tract and developmental disorders [14]. The causes of disability due to mobility problems in children may be cerebral palsy, congenital anomalies, orthopaedic, neurological and rheumatologic diseases, and conditions after injuries. Unfortunately, no standards for the prevention of rheumatic diseases in children have yet been developed.
The data discussed in our work come from the Electronic National Disability Assessment Monitoring System (EKSMoON), whose functionalities do not allow for a division into individual diseases. The symbol “05-R – musculoskeletal impairment” entered in the certificate covers jointly the following musculoskeletal disorders:
congenital and developmental defects of the musculoskeletal system,
systemic connective tissue diseases, depending on the period of the disease and the degree of functional capacity,
arthritis with accompanying spondylitis depending on the degree of functional capacity,
degenerative joint diseases depending on the degree of joint damage,
bone and cartilage diseases with impaired functional capacity,
neoplasms of the musculoskeletal system,
post-traumatic changes depending on the degree of damage and compensatory possibilities.
Among the above disorders, rheumatologists are professionally interested in systemic connective tissue diseases and arthritis with accompanying spondylitis. It is not possible to analyse the causes of disability in children aged 0–16 and to distinguish based on these aggregated data which children obtained a certificate due to congenital, post-traumatic and inflammatory defects. It is also impossible to obtain information without the consent of the parents whether these are first-time, subsequent or resulting from health worsening. A deeper analysis of the data is not possible because it would require access to medical records. Consent to the processing of personal data granted by persons receiving disability certificates does not cover this activity.
Adults are assessed according to three degrees of disability: mild, moderate and severe. In the case of children, there are no degrees of disability, only disability as such. Therefore, on the basis of anonymous data from EKSMoON, it is impossible to determine the percentage of people with significant, moderate or light deficits in a 0–16-year-old group. Determining these data is possible by analysing the indications entered in the disability certificates, but this requires access to the certificates, which is not possible due to the protection of personal data.
A separate issue is the controversies related to the indications included in the disability certificates. They determine the possibility for parents to obtain financial benefits, related to, for example, determining the need for permanent or long-term care or assistance of another person in connection with the significantly limited ability of the child to live independently. Another controversial issue is the expectations of parents regarding other data in the disability certificate, e.g. regarding the right to a parking card or the right to live in a separate room.
Sometimes the benefits resulting from having the disability certificate may result in a learned lack of independence. Unfavourable effects of having a disability certificate may develop in people who become largely dependent on financial benefits. After some time there can occur a medically confirmed improvement in health, rehabilitation brings the expected effects and one loses the disability certificate. It may be connected with loss of livelihood. Meanwhile, in Poland, following the example of Germany, there are occupational therapy workshops and sheltered workshops, whose task is to help young people on the verge of adulthood out of disability and find a place for them in the sheltered labour market. It is supposed to teach them self-reliance in adult life and independence from third parties [15].
Available systems, such as EKSMoON, contain data about disability certificates issued in individual years, and not the real number of disabled people. The number of certificates issued in a given year does not mean that there are X persons with disabilities in the area of operation of a given certification unit, because this number includes certificates issued once again due to the expiry of a temporary certificate, a change in the person’s health or a person’s transition from the category of children to the category of adults. In addition, the situation is complicated by the fact that the validity of some decisions has been extended under the COVID-19 epidemic regulations, so the health condition of people with “timely” decisions could radically change, they could die or they could change their place of residence.
The data about disabled citizens from EKSMoON, Statistics Poland, ZUS and KRUS differ as they are collected for different purposes.
Estimating the number of people with disabilities in Poland is possible on the basis of the results of the censuses. However, it should be noted that the censuses are organized approximately every 10 years, are based on voluntary responses, differ in methodology in individual years and introduce their own definition of disability (division into “legal” and “biological” disability). Consequently, the results of the censuses in individual editions differ drastically and at the same time do not indicate a reason for these differences.
Comparing Poland to other European countries poses similar difficulties. This is due to differences in defining disability, the approach to the phenomenon as such, and even economic and ideological reasons.
The highest disability rates for children aged 0 to 14 were reported in Australia, New Zealand and the United States, where the disability rate was estimated between 7% and 10.4%. By contrast, the lowest levels were reported in Mexico and Spain, with only 1.4% and 1.8%. In Germany 7.5% of males under the age of 25 and 5% of females that age live with disability. In Lithuania there were about 250,000 persons with disabilities (8% of the population). In this number there were about 15,000 children with disabilities [1]. In India there is 1 disabled child per 3 disabled adults and 1 geriatric patient, moreover 80% of the disabled individuals originate from rural areas and 20% from the cities. As many as 29% of disabled Indians suffer from post-traumatic deformity, 27% have post-polio paralysis, and 24% cerebral palsy or other congenital disorders. In India 45% of disabled people have mild, 30% moderate and 15% have severe disability [16].
The predominance of boys over girls in the group of children with issued disability certificates due to the musculoskeletal disorders probably results from the fact that boys that ages are more prone to injuries than girls [17].
From the rheumatologist’s point of view, rheumatic diseases in childhood can cause numerous problems in adulthood, such as: shortness, asymmetry of skeletal growth (which may require orthopedic interventions, orthopedic supplies, sticks, and even joint prostheses). A serious complication of juvenile idiopathic arthritis is cataract, glaucoma, and even blindness [17].
Another problem in caring for children with locomotor system diseases may be the shortage of specialists. Only 50 children’s rheumatologists work in Poland (with a population of 37.5 million people), and in the United States, 325 (with a population of 329.5 million) [16]. So there are 1.34 rheumatologists/1 million citizens in Poland and 0.98/1 million in the USA.
Many years of discussion on the adaptation of the International Classification of Functioning, Disability and Health (ICF) to the Polish system of certifying disability resulted in including this issue in the one adopted by the Council of Ministers in a document issued in 2021 entitled “Strategy for People with Disabilities 2021–2030”. According to this strategy, as a result of the announced reform of disability certificates issuance, the assessment of a person will be based on the ICF classification. The ruling will assess the individual needs of the opportunity and determine the extent of necessary support. It is also planned to merge the current institutions issuing disability certificates into one agency and to unify the rules. This will de facto abandon the system of certifying disability existing in Poland for a quarter of a century [6].
Conclusions
In children musculoskeletal problems are in the third position after diseases of the respiratory tract and developmental disorders as the reason for a disability certificate to be issued by a poviat/city in Poland.
These results are similar to those from developed countries.
Regardless of other factors (geographical, social), children constitute a population in which it is more difficult than in adults to collect full data on disability, both because of the methods of obtaining data directly from patients and proper reporting.
Also, the child population is not homogeneous and the assessment is hampered by the fact that it is divided into subjects over and under the age of 16 in terms of disability reporting methodology.