
Introduction
Idiopathic inflammatory myopathies (IIM) are a group of rare connective tissue diseases with incompletely elucidated pathogeneses. Several subtypes can be distinguished, including dermatomyositis (DM), polymyositis (PM), antisynthetase syndrome (AS), immune-mediated necrotizing myopathy (IMNM), overlapping myositis, cancer-associated dermatomyositis, and inclusion body myositis (IBM) [1, 2]. Lymphocytes, as key players of adaptive immunity, play a crucial role in the pathogenesis of IIM, contributing to both systemic inflammation and muscle tissue damage [3, 4]. Despite the flourishment of knowledge on circulating lymphocyte subpopulations and their importance for assessing disease activity and differentiating IIM subtypes [4], still little is known on the immunological mechanisms driving specific symptoms of IIM.
The aim of our study was to evaluate the profile of circulating lymphocytes in patients with IIM, and to determine whether imbalances in lymphocyte subsets are associated with clinical and serological phenotypes.
Material and methods
Study population
This was a single-center, cross-sectional study, conducted in the years 2021–2023. Out of the patients hospitalized in the Department of Rheumatology with Internal Disease Subdivision, USK no. 2 Hospital in Lodz, we recruited consecutive patients with IIM. The study group consisted of 40 participants with different subtypes of IIM. Inclusion criteria included: fulfilling the 2017 European Alliance of Associations for Rheumatology/American College of Rheumatology classification criteria for IIM or Solomon’s criteria for AS, age above 18 years, informed consent for participation; exclusion criteria were: concomitant active infection, congenital immunodeficiency disorders, inability to give informed consent for participation. A control group of 5 healthy individuals, without any autoimmune conditions or active infections, age- and sex-matched to the study population, was established to ensure the accuracy and reliability of the flow cytometry assessment.
Blood collection and separation of peripheral blood mononuclear cells
From study participants we collected 2 × 9 ml blood samples using heparin collection tubes (Sarstedt). Peripheral blood mononuclear cells (PBMCs) were subsequently isolated using the density gradient centrifugation method with Biocoll (Sigma Aldrich) separation reagent, following the manufacturer’s protocol. After isolation, the cells were counted using a Bürker counting chamber. Viability was assessed using the Trypan Blue exclusion test to determine the proportion of viable cells. The cells were then cryopreserved in a freezing medium composed of 10% dimethyl sulfoxide (DMSO) and a 1 : 1 mixture of RPMI-1640 medium and fetal bovine serum (FBS; Sigma Aldrich). Cryopreservation was carried out at –80°C using a controlled slow-freezing method in a cooling box to ensure gradual temperature reduction.
Cytometric assay
After quick thawing, the cells were washed with RPMI-1640 medium supplemented with 10% FBS and centrifuged to remove the 10% DMSO present in the freezing medium. Subsequently, cells were resuspended in the described medium. The cell suspension was incubated in a suspension culture flask for 2 hours at 37°C in a humidified incubator with 5% CO2. Viability and cell count methods were then assessed as described previously. For flow cytometric analysis, the BD Multi 6-Color TBNK assay (BD Biosciences) was used to phenotype lymphocyte subpopulations, including T cells, B cells, and NK cells, based on surface marker expression. T cells were defined as CD3+ cells, with CD4+ T cells identified as CD3+CD4+CD8– (helper T cells) and CD8+ T cells identified as CD3+CD4–CD8+ (cytotoxic T cells). Natural killer cells were defined as CD3–(CD16+ and/or CD56+)+CD19–, while B cells were defined as CD3–CD19+ cells. This gating strategy allowed for the identification and quantification of key lymphocyte subsets in the sample. The experiment was conducted using the CytoFLEX flow cytometer and software (Beckman Coulter). Additionally, cell viability was assessed using BD Horizon Fixable Viability Stain 510 (BD Biosciences), a fixable viability dye that discriminates live from dead cells by binding covalently to cell-surface and intracellular amines, with differential labeling depending on membrane integrity. This combination ensured precise immunophenotyping while excluding non-viable cells from the analysis, thereby preventing nonspecific antibody binding. The study was carried out at the Research Laboratory CoreLab of the Medical University of Lodz.
Statistical analysis
Data were analyzed statistically with STATISTICA 13 software. Normality of data was verified with the Shapiro Wilk test. Student’s t-test and the Mann-Whitney U test were used to compare variables with standard and non-standard distributions, respectively, between the studied groups.
Results
Characteristics of the study groups
Forty patients with IIM were included in the study. Mean age of the study group was 58.55 ±12.70 years, and most of the patients (n = 24, 60%) were females. Mean disease duration was 33 ±54.18 months with a mean diagnostic delay of 18.90 ±34.26 months. The majority of recruited patients had been diagnosed with AS (n = 14, 35%) or DM (n = 12, 30%). The most common clinical presentations included myositis (97.5%), arthralgia (55%), interstitial lung disease (ILD) (47.5%), and erythematosus skin lesions (42.5%). The patients presented with versatile serological profiles, with anti-Jo1, anti-PL7, and anti-Ro52 positivity being the most common ones. The most common comorbidities in the study group included hypertension, hyperlipidemia, and thyroid disorders. All but one of the patients were treated with glucocorticosteroids (GCs) at any stage of the disease, with the vast majority (90%) of patients receiving a combination of GCs and a GC-sparing agent. The most common GC-sparing agents used in the examined cohort were azathioprine, methotrexate, and intravenous immunoglobulins, which were received at any stage of the disease by respectively 67.5%, 27.5%, and 25% of the participants. Detailed characteristics of the studied populations are presented in Table I.
Table I
Characteristics of the studied populations
[i] AS – antisynthetase syndrome, AZA – azathioprine, CADM – cancer-associated dermatomyositis, CNI – calcineurin inhibitors, CQ/HCQ – chloroquine/hydroxychloroquine, DM – dermatomyositis, GCs – glucocorticosteroids, GERD – gastroesophageal reflux disease, IIM – idiopathic inflammatory myopathies, ILD – interstitial lung disease, IMNM – immune-mediated necrotizing myopathy, IS – immunosuppressive, IVIG – intravenous immunoglobulins, LEF – leflunomide, MMF – mycophenolate mofetil, MTX – methotrexate, OM – overlapping myositis, PM – polymyositis.
Comparison of study groups
The profile of circulating lymphocytes was assessed and compared between patients with IIM and healthy controls. Patients with IIM tended to have higher proportions of T cytotoxic cell and NK cell subpopulations, as well as a higher CD4+/CD8+ index, although this difference was not statistically significant. Detailed data on the differences in each subpopulation are presented in Table II. Patients with different IIM subtypes did not differ with respect to the distribution of circulating lymphocyte subpopulations.
Table II
Subpopulations of circulating lymphocytes compared between IIM group and control group
Lymphocyte subpopulations are associated with clinical phenotypes
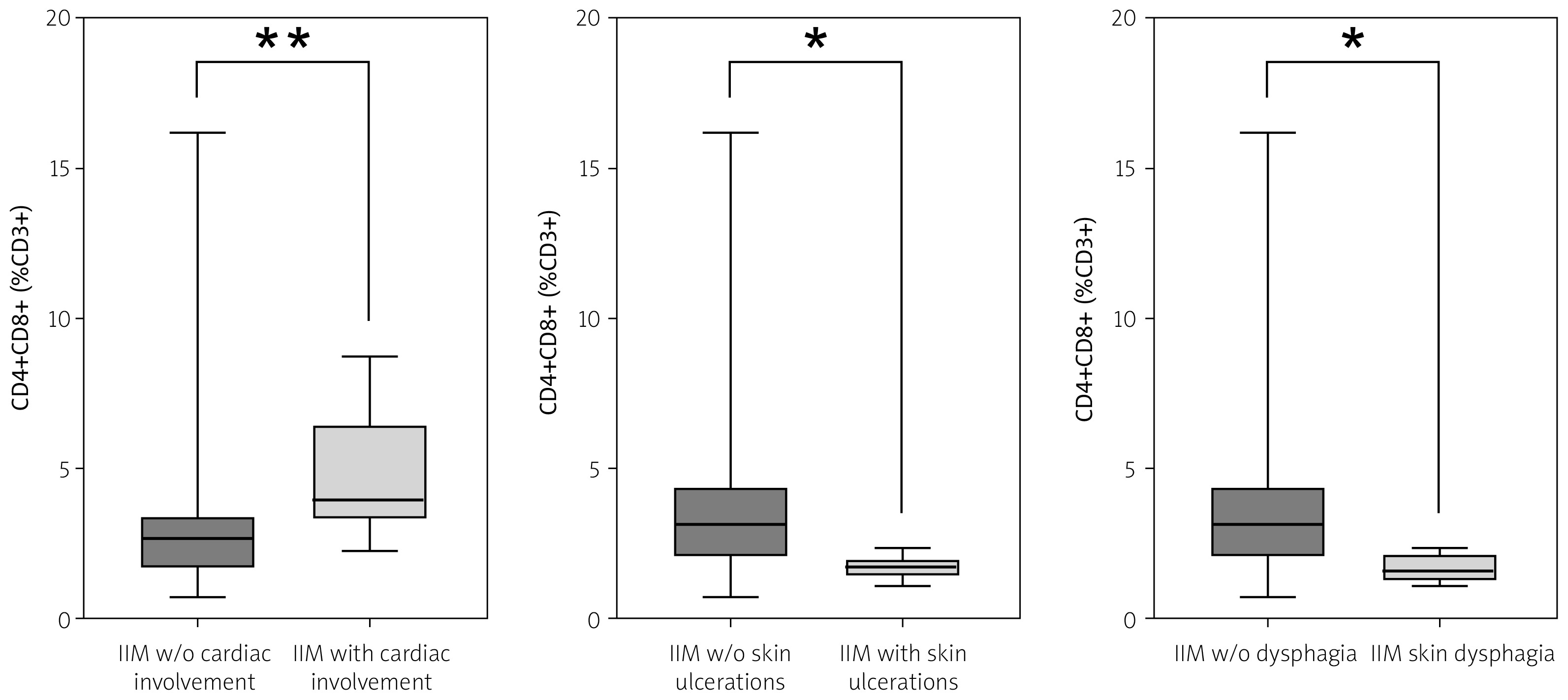
To analyze whether certain clinical symptoms were associated with imbalances in circulating lymphocyte subpopulations, we divided patients into subgroups according to the presence or absence of each of the clinical manifestations. Patients with cardiac involvement were found to present higher proportions of T cytotoxic cells (p = 0.0035), with median values of respectively 4.22 in patients with cardiac involvement and 2.65 in patients with no such complication. In patients with cutaneous ulcers, significantly lower proportions of double-positive CD4+CD8+ T cells (median of respectively 1.67 in individuals with skin ulcers vs. 3.14 in patients without cutaneous ulcers, p = 0.0480) were observed. Similarly, dysphagia was associated with lower proportions of CD4+CD8+ T cells (with medians of 1.67 vs. 3.17, p = 0.0183). No statistically significant differences were noted comparing patients with and without arthritis, Gottron’s sign/papules, heliotrope rash, non-specific erythematosus lesions, mechanic’s hands, Raynaud’s phenomenon, ILD, fever, and malignancy. Table III presents statistical comparisons of lymphocyte distribution according to clinical phenotypes. Figure 1 presents significant abnormalities.
Table III
P-values from Mann-Whitney U tests, comparing the proportions of lymphocyte subpopulations in patients with and without specific clinical symptoms
Lymphocyte subpopulations are associated with serological profiles
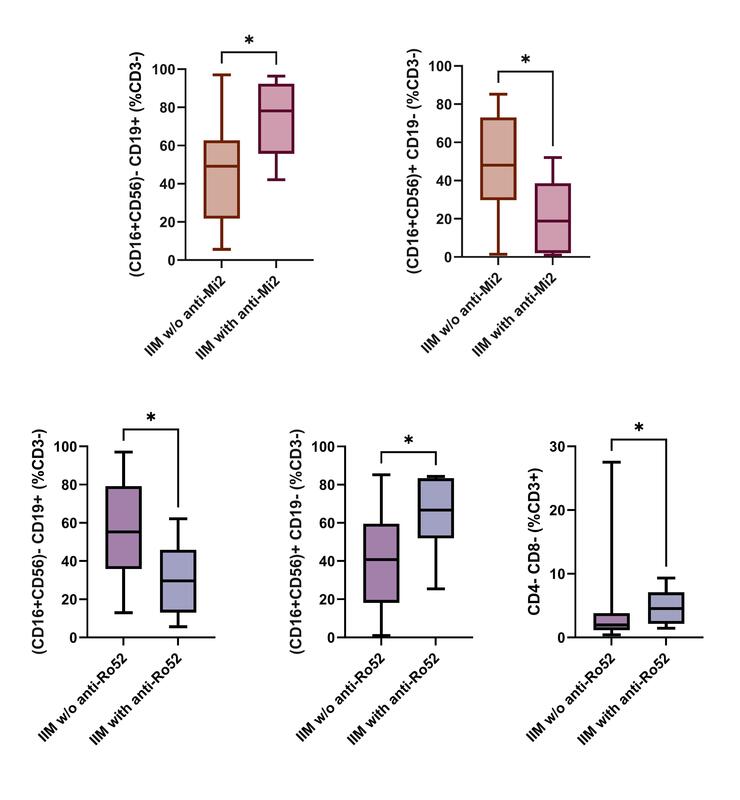
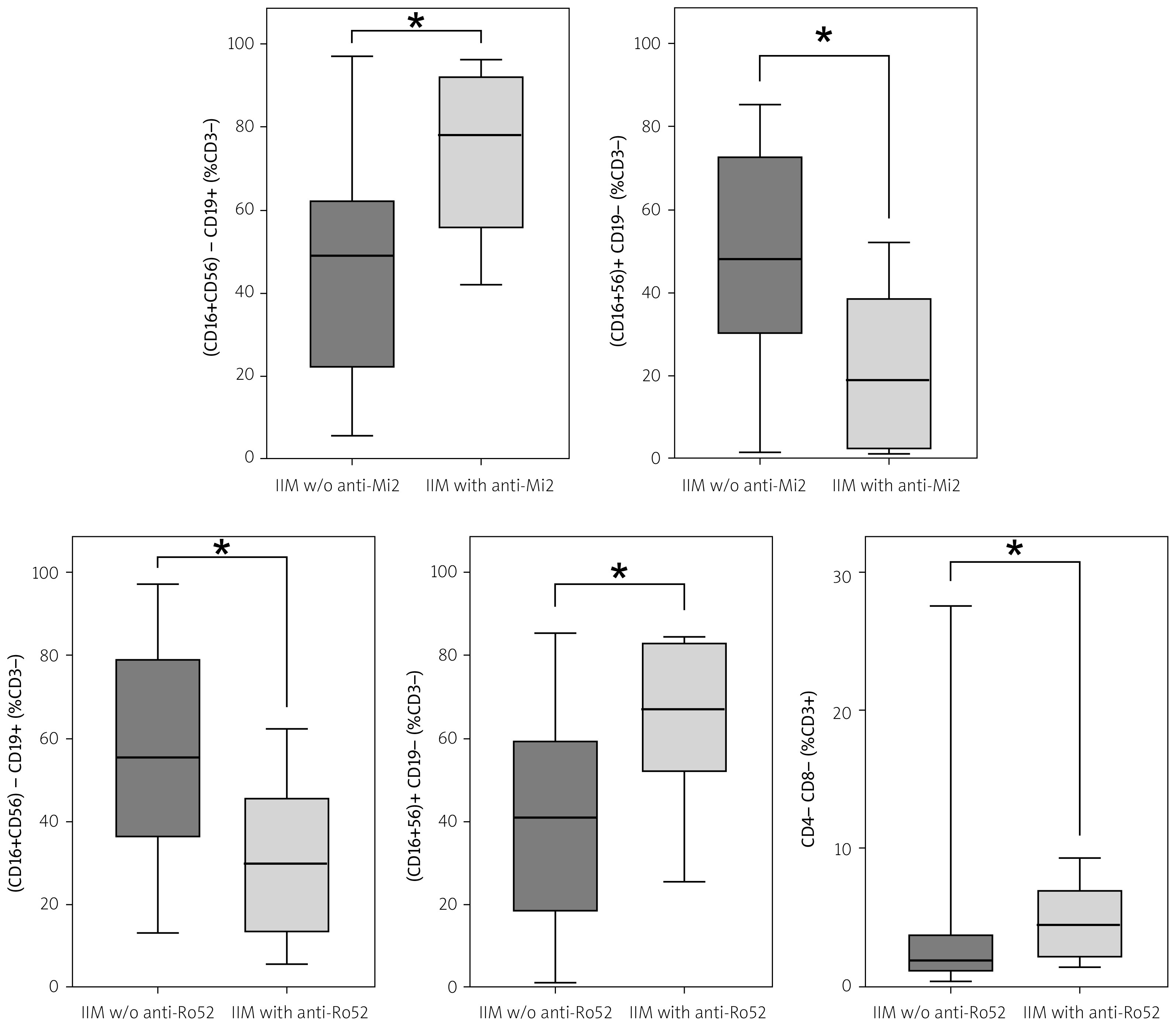
To analyze whether certain serological profiles were associated with altered composition of peripheral lymphocytes, we divided patients into subgroups according to the presence or absence of specific antibodies. Due to the low prevalence of some of the antibodies in our cohort and therefore potential risk of bias, subgroups with less than 3 patients were excluded from further analysis. Patients with anti-Mi2 antibodies were characterized by significantly lower proportions of NK cells (median value of 18.82 in anti-Mi2 positive patients vs. 48.05 in anti-Mi2 negative group, p = 0.0169) and significantly higher proportions of B cells (median values of respectively 78.11 vs. 49.12, p = 0.0213). In contrast, the opposite pattern was observed in patients with anti-Ro52: NK cells were significantly higher (median value of 66.68 in anti-Ro52 positive patients vs. 40.79 in anti-Ro52 negative group, p = 0.0121), while proportions of B cells were significantly lower (median values of respectively 29.59 vs. 55.33, p = 0.0109). In patients with anti-Ro52, the median prevalence of double negative T cells (CD4–CD8– population) was elevated as compared to anti-Ro52 negative patients (respectively 4.55 vs. 1.96, p = 0.0465). Table IV presents statistical comparisons of peripheral lymphocyte composition, according to serological profiles. Figure 2 presents significant abnormalities.
Table IV
P-values from Mann-Whitney U tests, comparing the proportions of lymphocyte subpopulations in patients with and without specific antibodies
Impact of treatment on peripheral blood mononuclear cell subpopulations
As iatrogenic suppression of the immune system may correspond to alterations in the PBMC profile, we analyzed the changes in lymphocyte subpopulations according to the administered treatment. As all the patients received GCs, the impact of GCs on PBMC changes was not evaluated. At the time ofblood collection, none of the patients had a history of treatment with rituximab. For the remaining treatment modalities, no significant differences were noted.
Lymphocyte subpopulations are associated with the risk of death
Electronic medical records were retrospectively reviewed at the moment of data analysis, revealing that 6 of the 40 patients had died since the beginning of the study (3 patients with AS, 1 patient with IMNM, 1 patient with PM, and 1 patient with OM). Profiles of circulating lymphocyte were compared between the deceased and surviving patients. No differences in the basic subpopulations of lymphocyte subsets were noted.
Discussion
Lymphocytes, as key players of adaptive immunity, ensure defense against pathogens and harmful agents, but also form a network of intricate connections between the immune system and the remaining cells in our bodies. Such a heterogeneous spectrum of action is possible due to the specialization of lymphocytes into distinct subtypes, each with specific roles. Disturbances in the proper functioning or composition of lymphocytes can lead to autoimmunity. So far, several studies have assessed the profile of circulating lymphocytes in IIM, but the results remain inconclusive.
In 1 of the earliest studies in this field, lower proportions of CD8+ and higher proportions of CD3+ and CD14+ cells were noted in the IIM group as compared to healthy controls [5]. Patients with untreated juvenile dermatomyositis (JDM) exhibited lower total lymphocyte counts with decreased proportions of CD3+, CD4+, and CD8+ [6]. In the DM population, higher proportions of naïve CD4+ T cells were noted, whereas naïve CD8+ T cells, central memory CD8+ T cells, effector memory CD4+ T cells, Th1 cells, and follicular helper T cells were less abundant compared to healthy donors [7]. Espinosa-Ortega et al. deepened the analysis of T cell subsets in IIM, observing a significant increase in follicular helper T cells (CD4+CXCR5+), type 17 T cells (CD4+IL17A+), and pro-apoptotic CD28null cells (CD4+CD28-CD244+), as well as decreased proportions of regulatory T cells (CD4+CD25highFOXP3+; CD8+CD25highFoxP3+) [8]. Peripheral helper T cells are a recently identified subpopulation of T cells that were found to be decreased in the blood of DM patients and abundant in muscle tissue infiltrates, suggesting their crucial role in DM pathogenesis [9]. However, the exact mechanisms of their involvement are unclear, as Treg activation in DM was found to be comparable to healthy controls [10]. In our study, the overall proportions of main T cell subsets remained comparable to healthy individuals; however, we did not analyze specific subsets of CD4+ and CD8+ cells.
According to Wang et al. [11], patients with IIM were characterized by elevated total CD19+ B cells with elevation in the naïve B cell population and a decrease in the memory B cell subsets. Their results align with another study, which also reported a significant increase in CD19+ B cells in IIM patients, with overexpression of naïve B cells and a significant decrease in memory B cells and double-negative B cells [12]. Similarly, in the DM population assessed by Sasaki et al. [7], naïve B cells were more prevalent compared to memory B cells [7]. In the above-mentioned juvenile population, the relative percentages of CD4+ and CD19+ were notably higher in JDM, while the relative percentage of CD8+ was significantly lower than in healthy controls, supporting the hypothesis of humoral-drive mechanisms in JDM [6]. Recently, regulatory B cells are gaining recognition as the crucial players underlying inflammation in IIM. Compared to both healthy individuals and patients with other autoimmune conditions, patients with DM were found to present significant deficiency of the CD19+CD24highCD38high Breg population, which improved after achieving remission [13]. Our results did not confirm an imbalance in the total B cell proportions in IIM. The percentage of the (CD16+CD56)–CD19+ subpopulation did not differ between IIM and healthy individuals; however, as we did not assess any specific subsets of B cells, we could not exclude potential differences which are lost when analyzing B cells in total.
In our study, no statistically significant differences in the basic lymphocyte profiles were noted between the subtypes of IIM. This is in line with the study by Viguier et al. [14]. However, in a larger study using high-dimensional flow cytometry, several unique features were identified for some of the IIM subtypes. In patients with IBM, terminally differentiated cytotoxic CD8 T cells were significantly higher than in other subtypes. A shift of CD4+ T cells towards effector memory cells was noted in patients with AS, but not in other IIM subtypes. As for the B cells, patients with AS were found to have higher proportions of naïve B cells and lower proportions of switched memory B cells [15]. This is in line with another study, which demonstrated a reduction in the circulating memory B cells with an increase in the proportion of peripheral naïve B cells in AS patients, compared to other IIM subtypes and healthy controls. Notably, muscle biopsies of AS patients confirmed infiltrations of memory B cells, suggesting the translocation of this lymphocyte subset to the muscle milieu [16]. Miller et al. [5] reported that DM patients could be distinguished from PM and IBM based on an elevation in the peripheral CD20+ subpopulation and a decrease in CD3+DR+ cells. In 1 of the studies, both DM and PM patients showed significant increases in CD19+, CD19+, CD23+ cells as well as a decrease in memory T cells, whereas other abnormalities were DM or PM specific only (the decrease in the CD4+ CD45RO+/CD4+ CD45RA+ ratio was limited to DM; a decrease in CD3+ CD4+ cells was observed only in PM) [17]. As we evaluated only the basic subsets of circulating lymphocytes, we cannot exclude the possibility of potential differences in non-assessed detailed subsets of T or B cells also in our cohort.
So far, the association of circulating lymphocyte subpopulations with clinical phenotypes has been rarely evaluated in IIM. Patients with ILD in the course of AS were found to have lower CD8+ counts, a higher proportion of Th17, and an elevated Th17/Treg ratio, supporting the hypothesis of the crucial role of T helper cells and peripheral Th17/Treg imbalance in the pathogenesis of AS-ILD [18]. Similarly, in a Chinese cohort, elevated CD4+CXCR4+ proportions were found in patients with IIM-ILD, which correlated with severity of ILD and higher mortality [19]. In contrast, in another Asian study, decreased CD3+ cell counts and percentages of CD3+CD4+ cells were associated with ILD in the course of DM/PM [20]. Further studies are needed to clarify how the observed abnormalities in T cells correspond to the risk of ILD in different IIM subsets. T cells are not the only ones involved in the pathogenesis of interstitial lesions in IIM. A Breg deficiency was noted in individuals with DM-ILD [13]. The total NK cell count was reduced in patients with IIM-associated pulmonary involvement, with CD56dim NK cells contributing strongly to the observed imbalance. Furthermore, significant alterations in the cell receptors on NK cells were observed, serving as a plausible marker for pulmonary complications [21]. In our cohort, we did not observe any imbalance in lymphocyte subpopulations in patients with ILD; however, as we assessed only the main subsets, we cannot exclude the possibility of missed associations with certain specific subsets. According to the literature, patients with IIM-associated rash exhibited lower proportions of non-switched memory B cells as compared to patients without rashes [11]. We did not evaluate the subsets of naïve and memory B cells in our patients. To our knowledge, the association with other clinical manifestations has never been investigated before. We observed that patients with cardiac involvement exhibited a significantly elevated CD4+CD8+ T-cell subpopulation. Furthermore, abnormally low proportions of the CD4+CD8+ T-cell subset were noted in patients with skin ulcerations and dysphagia. As no differences in the proportions of circulating lymphocytes were noted between the IIM subtypes, we conclude that the observed abnormalities should be considered symptom-specific.
Double-positive T cells (CD4+CD8+), which were found to be unbalanced in our cohort, are a fascinating subset of cells with incompletely elucidated origin and functions. As a significant proportion of peripheral double-positive T cells does not express typical thymic markers, their occurrence cannot be entirely explained by disturbed selection in the thymus. This subpopulation was found to be abnormally present in targeted organs of several autoimmune conditions including systemic sclerosis, rheumatoid arthritis, and adult-onset Still’s disease [22]. To our knowledge, this subpopulation has never been associated with clinical symptoms of IIM. In our study, abnormalities in this subset were observed in patients with cardiac involvement, dysphagia, and cutaneous ulcers. Assessing the infiltrates in affected organs could shed light on the role of double-positive T cells in IIM.
In recent years, there has been a tendency to divide IIM according to the serological profile. We found that the proportion of circulating (CD16+CD56)+CD19– NK cells was significantly elevated in patients with anti-Ro52 antibodies and significantly decreased in patients with anti-Mi2 antibodies. B cells (CD16+CD56)–CD19+ were found to be significantly elevated in individuals with the anti-Mi-2 profile and notably decreased in the anti-Ro52 population. Furthermore, double-negative T cells (CD4–CD8–) were found to be elevated in the presence of anti-Ro52 antibodies. The association of lymphocyte subpopulations with serological profiles has been noted in a few previous studies. Patients with anti-Jo-1 antibodies were characterized by higher proportions of CD20+ cells but lower proportions of CD3+ and CD4+ cells and a lower CD4/CD8 ratio, according to Miller et al. [5]. The proportion of regulatory B cells was decreased in patients with myositis-specific autoantibodies (MSA) [13]. Abnormalities in the lymphocyte profile seem to be exceptionally frequent in patients with anti-MDA5 antibodies. In a Chinese cohort, an NK cell imbalance was found in patients with anti-MDA5 antibodies. In this population, significantly lower NK cell levels correlated with higher disease activity and an unfavorable prognosis [23]. In another study, patients with anti-MDA5 antibodies were characterized by a higher proportion of CD19+ B cells [11]. As regards the T cell repertoire in anti-MDA5 positive DM, the proportions of naïve CD4+ T cells, naïve CD8+ T cells, CD38+CD4+ T cells, and CD38+CD8+ T cells were significantly higher compared to healthy controls, while the proportions of central memory CD4+ T cells and CD8+ T cells were significantly lower. Moreover, elevated CD38+CD4+ and CD38+CD8+ subpopulations were mostly expressed in patients with rapidly progressive ILD [24]. In our study, only 2 patients were anti-MDA5 positive, which limited reliable assessment. The low prevalence of anti-MDA5 antibodies in our cohort aligns with the prevalence observed in other European studies [25].
Double negative T cells (CD4–CD8–) are an intriguing population, which have been proven to exert double-edged sword-like effects in distinct settings. These lymphocytes may act as suppressors of activated T helper, T cytotoxic, or B cells, but also secrete effector or proinflammatory cytokines including interleukin-17, tumor necrosis factor, and interferon-γ, thereby promoting autoimmunity or tumorigenesis [26]. The role of double negative T cells is well documented in systemic lupus erythematosus, antiphospholipid syndrome, Sjögren’s disease and psoriasis but has so far not been explored in IIM [27]. In our study, we found a significantly higher percentage of the CD4–CD8– population in patients with anti-Ro52 antibodies. As those antibodies are also frequently observed in patients with other autoimmune conditions, we conclude that this subset of lymphocytes may be involved in promoting anti-Ro52 secretion.
So far, only a few studies have evaluated the association of lymphocyte profile with the risk of death. According to the literature, lower proportions of CD3+CD8+ cells should be considered a risk factor for death [20]; however, our study did not confirm this.
Study strengths and limitations
Our study provides valuable and novel insights into the association of peripheral lymphocytes with clinical and serological profiles in IIM patients. In the era of personalized medicine, understanding the exact immunological mechanisms underlying certain symptoms is crucial for adjusting the most suitable therapy for each individual. However, our study has several limitations that may influence the interpretation of the results. First, disease activity was not assessed in our cohort. The recruited patients were at different stages of the disease. However, as demonstrated in the study by Ernste et at. [28], the median percentages of almost all basic lymphocyte subpopulations in JDM (except for CD16+CD56+) did not change over time and remained comparable after an average of 9 months. Moreover, patients in our cohort were receiving various immunosuppressive therapies, which may have altered the profiles of circulating lymphocytes. However, Miller et al. [5] noted that GCs administered over 24 hours prior to the study did not change the cell counts. As all of the patients in our cohort received GCs, the impact of those drugs was impossible to evaluate. In our patients we also evaluated whether treatment modalities impacted the profiles of circulating lymphocytes, and we found no alterations.
Conclusions
Characterization of the circulating lymphocyte profile provides critical insights into the immune dysregulation in IIM and offers valuable tools for disease monitoring and management. Abnormalities in the circulating lymphocytes are associated with specific clinical and serological presentations. Assessing the basic profile of peripheral lymphocyte in IIM may be a useful and readily available tool to predict complications and disease outcome.