
Introduction
Fibromyalgia (FM) is one of the most common causes of chronic widespread pain and the second most common rheumatic disease after osteoarthritis [1]. Fibromyalgia can cause extremely negative physical effects on patients. Many patients are physically incapacitated, have reduced physical functions, and have a significantly impaired quality of life [2, 3].
The term “core” refers to the trunk and more specifically to the lumbopelvic region of the body [4]. The “core” includes the proximal lower extremity, proximal upper extremity, hip, pelvis, and spine [5]. The “core” region provides a stable basis for the action of peripheral muscles. Since the strength required for the formation of movements is produced by the “core” region and transmitted from the proximal segments to the distal segments, this region forms the basis of the extremity movements [6].
Studies have indicated that “core” stabilization has an effect on upper and lower extremity functions [7, 8]. Core stabilization, which provides a basis for movements, has a very important role in the transmission and distribution of strength from the extremities to the core and from the core to the extremities along the kinetic chain. By performing the “core” functions at the best level, dynamic joint stability is provided along the kinetic chain and safe and efficient movement formation away from the “core” region is supported. Stabilization of the proximal body segments is necessary for the continuity of the functions and mobility of the distal body segments [5]. Core endurance allows the core stabilization over long periods of time. Maintaining core muscle endurance is considered important for performance, because it enables us to perform daily living and sports activities with ease [9]. The decrease in the endurance of the core muscles causes physiological stress in the passive structures of the spine. This can cause pain in the body and reduce functional performance [10].
Since FM is a chronic disease with widespread pain and fatigue in the body, muscle strength and endurance are negatively affected and trunk muscle endurance is also reduced [11, 12]. A decrease in the strength/endurance of the abdominal and lower back muscles is observed in individuals with FM. Decreased muscle strength/endurance can lead to decreased functional capacity [13]. Upper and lower extremity physical performance capacities are reduced, and this situation affects the independence of individuals in their daily living activities [14].
In the literature, studies examining the relationship between “core” stabilization and extremity functions focus more on athletes and healthy young individuals, and they are also studied in certain disease populations (especially low back pain) [15, 16]. This is the first study to examine the relationship between core stabilization and limb functional status in individuals with FM.
The incidence of FM increases with age and is higher in women than in men at all ages [1]. Therefore, we aimed to examine the relationship between the functional status of the extremities, aerobic capacity and pain with “core” stabilization in women with FM.
Material and methods
Participants
The study included 57 women with FM who were followed up by the Department of Rheumatology, Pamukkale University hospital, and diagnosed with FM by the same rheumatologist according to the FM classification criteria of the 2016 American College of Rheumatology.
Inclusion criteria: diagnosed with FM by the same rheumatologist according to the FM classification criteria, aged between 18 and 65 years, sex – female, volunteered to participate in the study.
Exclusion criteria: presence of carpal tunnel syndrome, polyneuropathy, malignancy, another disease, concurrent autoimmune or inflammatory disease, being pregnant, had surgery on the upper or lower extremities in the last 6 months.
Evaluations
Evaluations for all participants were made by the same researcher using the face-to-face interview method in an environment where the same conditions were met. Each appointment took approximately 50 minutes. Pain was evaluated with the Widespread Pain Index (WPI) and Visual Analogue Scale-Pain (VAS-Pain), symptom severity with the Symptom Severity Scale (SSS), functional status with the Fibromyalgia Impact Questionnaire (FIQ), core stabilization with McGill Static endurance tests (trunk flexors endurance test, trunk extensors endurance test (Biering-Sorensen test) and lateral bridge test), upper extremity functions with the Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH), grip strength with with electronic hand dynamometer; lower extremity functions with the Lower Extremity Functional Scale (LEFS) and chair-stand test, pressure pain threshold with a pressure algometer (Commander Echo), and aerobic capacity with the 6-minute walk test (6MWT).
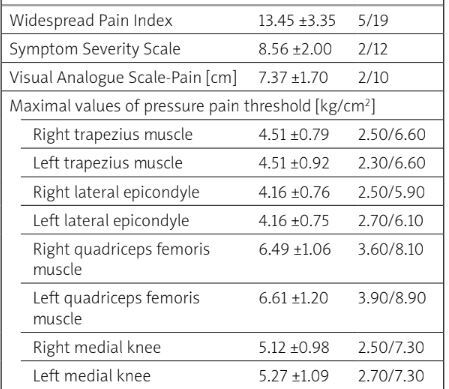
Widespread pain index and symptom severity scale: The widespread pain index quantifies the patient’s pain in terms of 19 regions. The score is calculated as a result of stating the painful areas in the last week. The total score is between 0 and 19. The symptom severity scale is scored between 0 and 12. A higher score means more symptoms and more pain [17].
Visual Analogue Scale-Pain (VAS-Pain): The Visual Analogue Scale, which measures pain severity in one dimension, is a valid and reliable scale. In the present study, the pain intensity of the patient in the last week was evaluated with the VAS. A score of “0” means “no pain”, while “10” means “unbearable pain” [18].
Pressure pain thresholds: Pressure pain threshold measurements were evaluated using a pressure algometer (JTECH Medical Commander Echo, Midvale, UT, USA). The tender points evaluated were the trapezius muscle, elbows (lateral epicondyle), quadriceps femoris muscle and medial knee (in the medial fat pad close to the joint line). Three measurements were made at a total of 8 tender points. The reading was expressed in kg/cm2. Two results were obtained as maximal values and mean values of the pressure pain threshold for each point [19].
Fibromyalgia Impact Questionnaire: developed by Burchardt et al. to measure functional status in FM patients. This questionnaire measures 10 different characteristics (physical impairment, days felt good, work missed, work impairment, pain, fatigue, morning tiredness, stiffness, anxiety, and depression) and consists of 10 questions. A maximum of 100 points can be obtained for this questionnaire consisting of 10 questions. A high score indicates worsening functional status [20].
McGill Static Endurance Tests
Trunk flexors endurance test: The patient lies on her back with the hips and knees flexed to 90°, the arms crossed over the chest on the opposite shoulders, and the feet in a fixed position. The test begins in a supported sitting position with the trunk 60° flexed. The trunk support is then removed and the patient is asked to maintain this position as much as possible. The test ends when the 60° angle between ground and upper body changes and the time is recorded in seconds.
Trunk extensors endurance test (Biering-Sorensen test): The patient lies on the bed in the prone position with the iliac cristae aligned at the bedside. The pelvis, hips and knee are fixed to the bed. The trunk and upper extremities are supported by a chair. Then, the chair is retracted and the patient is asked to maintain the horizontal position of the trunk for as long as possible while the arms are crossed over the chest. The test ends when horizontality is broken. The time is recorded in seconds.
Lateral bridge test: The patient lies on her side on a bed with the legs extended. The top foot is placed in front of the bottom foot for support. The upper arm is placed on the opposite shoulder, crossing the chest. The lower elbow joint is placed in the flexion position, so that it can receive support from the elbow and forearm. Patients raise their hips and knees off the ground so that the whole body forms a straight line. The test ends when the position is lost and the time is recorded in seconds. In the present study, the test was performed bilaterally [21].
Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH): The DASH measures disability, symptoms and activities of daily living of upper limb disorders and contains thirty items. The total score varies between 20 and 100, and the higher the score, the higher the level of disability [22].
Grip strength: A electronic hand dynamometer (Baseline evaluation instruments, model 12-0286) was used to measure the grip strength. The patient sat in a chair with a back support and no arm support, with both feet on the floor on a flat surface. The shoulder was positioned in neutral, the elbow in 90° flexion, and the forearm in neutral rotation [23]. Measurements were made bilaterally 3 times. One-minute rest intervals were given between each measurement and the mean value was recorded in kg.
Chair-stand test: Lower extremity muscle strength and functional performance were evaluated with the sit-to-stand test. In the starting position of the test, the patient’s arms are crossed in front of the body and their feet are in full contact with the ground. Patients are asked to sit and stand as fast as they can for 30 seconds from a standard chair with back support and no arm support. Full take-off sits are recorded [24].
Lower Extremity Functional Scale: The scale evaluates a person’s ability to perform everyday tasks and consists of 20 questions. Each question is scored between 0 and 4. A total of 0–80 points can be obtained. Higher scores indicate better functional status [25].
The 6-minute walk test: The 6-minute walk test was used to evaluate the aerobic capacity of the patients. It was developed by the American Thoracic Society and it is safe, easy to apply and reflects the daily life activities of the patients well. In a 30 m long straight corridor, under the supervision of a physiotherapist, the patients were asked to walk as long as possible in their own rhythm and with standard commands for 6 minutes. Distance walked after 6 minutes was recorded in meters [26].
Statistical analysis
The effect size, depending on the FIQ parameter, from the reference study was moderate (r = 0.365). As a result of the power analysis, it was calculated that 80% power could be obtained at the 95% confidence level when at least 54 patients were included in the study [27]. Data were analyzed with the SPSS 25.0 package program. Continuous variables were given as mean ± standard deviation, and descriptive categorical variables were given as numbers and percentages. Relationships between continuous variables were analyzed by Pearson correlation analysis for normally distributed data and Spearman correlation analysis for non-normally distributed data. The significance level was accepted as p ≤ 0.05. Correlations were interprested as follows: r < 0.2 was very weak, r = 0.2–0.4 was weak, r = 0.4–0.6 was moderate, r = 0.6–0.8 was strong, and r > 0.8 was very strong. Multivariate multiple regression was used to identify the major variables influencing the dependent variable (“core” stabilization tests) and rank them in order of importance.
Bioethical standards
Ethics committee approval was obtained for the study from the non-interventional clinical research Ethics Committee of Pamukkale University at the committee meeting numbered E-60116787-020-86558 (date: 3 August 2021; decision no: 14). All individuals were informed verbally and informed consent forms were signed. This study was conducted in accordance with the Declaration of Helsinki.
Results
The mean age of women with FM was 43.91 ±10.50 years, and the mean disease duration was 4.00 ±4.68 years. There were 6 patients with an exercise habit and 51 patients without. According to these results, the majority of the patients were sedentary. Demographic and disease-related data are shown in Table I, and descriptive data of evaluations are shown in Table II.
Table I
Demographic and disease-related data of women with FM
Table II
Descriptive data of evaluations of women with FM
The relationship of core stabilization with upper and lower extremity functional status
The trunk flexors endurance test showed a weak correlation with 6MWT (r = 0.392, p = 0.003), DASH (r = –0.347, p = 0.008) and LEFS (r = 0.328, p = 0.013; Table III).
Table III
The relationship of core stabilization with upper and lower extremity functional status in women with FM
| Variables | FIQ | Grip strength (right) | Grip strength (left) | Chair-stand test | 6MWT | DASH | LEFS | |
|---|---|---|---|---|---|---|---|---|
| Trunk flexors endurance test | r | –0.107 | 0.252 | 0.247 | 0.150 | 0.392 | –0.347 | 0.328 |
| p | 0.43* | 0.06* | 0.06* | 0.26v | 0.003v | 0.008* | 0.013* | |
| Trunk extensors endurance test | r | –0.191 | 0.285 | 0.407 | 0.470 | 0.524 | –0.301 | 0.321 |
| p | 0.15v | 0.032v | 0.002v | 0.001v | 0.001v | 0.023v | 0.015v | |
| Right lateral bridge test | r | –0.077 | 0.271 | 0.418 | 0.194 | 0.414 | –0.379 | 0.254 |
| p | 0.56v | 0.042v | 0.001v | 0.148v | 0.001v | 0.004v | 0.05v | |
| Left lateral bridge test | r | –0.060 | 0.279 | 0.502 | 0.276 | 0.359 | –0.294 | 0.221 |
| p | 0.66v | 0.036v | 0.001v | 0.038v | 0.007v | 0.026v | 0.098v | |
The trunk extensors endurance test showed a weak correlation with grip strength-right (r = 0.285, p = 0.032), DASH (r = –0.301, p = 0.023) and LEFS (r = 0.321, p = 0.015); it showed a moderate correlation with grip strength-left (r = 0.407, p = 0.002), chair-stand test (r = 0.470, p = 0.001) and 6MWT (r = 0.524, p = 0.001; Table III).
The right lateral bridge test showed a weak correlation with grip strength-right (r = 0.271, p = 0.042), DASH (r = –0.379, p = 0.004) and LEFS (r = 0.254, p = 0.05); it showed a moderate correlation with grip strength-left (r = 0.418, p = 0.001) and 6MWT (r = 0.414, p = 0.001; Table III).
The left lateral bridge test showed a weak correlation with grip strength-right (r = 0.279, p = 0.036), chair-stand test (r = 0.276, p = 0.038), 6MWT (r = 0.359, p = 0.007), DASH (r = –0.294, p = 0.026); it showed a moderate correlation with grip strength-left (r = 0.502, p = 0.001; Table III).
The relationship between “core” stabilization and pain
The trunk flexors endurance test showed a weak correlation with WPI (r = –0.289, p = 0.029; Table IV).
Table IV
The relationship between “core” stabilization and pain in women with FM
| Variables | VAS-Pain | WPI | SSS | Pressure pain threshold | ||
|---|---|---|---|---|---|---|
| Average of maximal values | Average of mean values | |||||
| Trunk flexors endurance test | r | –0.089 | –0.289 | –0.045 | 0.205 | 0.213 |
| p | 0.511* | 0.029* | 0.738v | 0.127v | 0.112* | |
| Trunk extensors endurance test | r | –0.162 | –0.243 | –0.110 | 0.131 | 0.153 |
| p | 0.227v | 0.068v | 0.415v | 0.331v | 0.255v | |
| Right lateral bridge test | r | –0.053 | –0.306 | –0.088 | 0.316 | 0.337 |
| p | 0.694v | 0.020v | 0.516v | 0.017v | 0.010v | |
| Left lateral bridge test | r | –0.016 | –0.175 | –0.038 | 0.315 | 0.370 |
| p | 0.904v | 0.192v | 0.777v | 0.017v | 0.005v | |
The right lateral bridge test showed a weak correlation with WPI (r = –0.306, p = 0.020), average of maximal values of pressure pain threshold (r = 0.316, p = 0.017) and average of mean values of pressure pain threshold (r = 0.337, p = 0.010; Table IV).
The left lateral bridge test showed a weak correlation with average of maximal values of pressure pain threshold (r = 0.315, p = 0.017) and average of mean values of pressure pain threshold (r = 0.370, p = 0.005; Table IV).
Multivariate multiple regression
Multivariate multiple regression was used to identify the major variables influencing the dependent variable (“core” stabilization tests). For the trunk flexors endurance test, 6MWT was a significant predictor variable and explained 80.8% of the total variance. For the trunk extensors endurance test, grip strength-left was a significant predictor variable and explained 71.4% of the total variance. For the right lateral bridge test, grip strength-left was a significant predictor variable and explained 51.2% of the total variance. For the left lateral bridge test, grip strength-left was a significant predictor variable and explained 56.7% of the total variance (Table V).
Table V
Results of multivariate multiple regression analysis for variables predicting core stabilization
| B | SE | Beta | t | 95% CI (lower/upper) | F | R | R2 | DW | |
|---|---|---|---|---|---|---|---|---|---|
| Trunk flexors endurance test | |||||||||
| 6MWT | 0.037 | 0.002 | 0.899 | 15.211* | (0.032/0.041) | 231.37* | 0.899 | 0.808 | 2.162 |
| Trunk extensors endurance test | |||||||||
| Grip strength-left | 0.128 | 0.096 | 0.845 | 11.727* | (0.936/1.321) | 137.52* | 0.845 | 0.714 | 1.738 |
| Right lateral bridge test | |||||||||
| Grip strength-left | 0.393 | 0.052 | 0.715 | 7.593* | (0.289/0.496) | 57.65* | 0.715 | 0.512 | 1.818 |
| Left lateral bridge test | |||||||||
| Grip strength-left | 0.551 | 0.065 | 0.753 | 8.491* | (0.421/0.681) | 72.10* | 0.753 | 0.567 | 1.830 |
Discussion
In the present study, core muscle endurance is associated with upper and lower extremity functional level, aerobic capacity, and pain parameters in women with FM. While lower extremity functionality was related especially to core extensor muscles, both core extensor and core lateral muscle endurance were found to be related to upper extremity functionality (especially left side). In addition, women with FM who had less core flexor and lateral (especially right) muscle endurance felt pain more intensely and had lower pressure pain thresholds.
Studies have shown that individuals with FM have lower muscle strength and performance than healthy individuals, and as a result, their functional abilities and extremity physical performance capacities are reduced. Evaluation of functional performance in FM patients is important to understand its relationship with health factors [14, 28].
The core region is actually a 3-dimensional space surrounded by muscles: diaphragm (superior), abdominal (anterior), oblique muscles (lateral), paraspinal and gluteal muscles (posterior), and pelvic floor and hip girdle (inferior) [29]. Three core stability tests are widely used by clinicians (right and left lateral bridge, trunk flexor endurance and extensor endurance tests) [21]. Therefore, McGill static endurance tests were used to evaluate core stabilization in the present study.
The core is the region that connects the upper and lower extremities [30]. At the beginning of the movements, the muscles in the core region are activated and the strength resulting from this contraction is transmitted to the extremities [5]. “Core” stabilization has a role in limb mobility and functional performance, and affects limb functionality [31, 32]. The relationship between “core” stabilization and extremities can be described as follows: the stabilization of the proximal segments must be provided for the mobility of the distal segments and the continuity of their functions. Good stabilization in the proximal region increases the quality of movement and performance of the distal segments [5].
Many studies have emphasized that core stability affects upper and lower extremity functionality. Inadequate core muscle endurance leads to inhibition of specific extremity muscles [33, 34]. However, there is no clarity as to which muscle group is more important for which extremity [35]. In the present study, it was found that all core muscle endurance values were related to upper and lower extremity functionality. However, the core extensor muscle group showed the strongest relationship with lower and upper extremity functionality. Core lateral muscle endurance in addition to core extensor muscle endurance was found to be related to DASH and grip strength right and left. But the endurance of these muscles showed a stronger correlation especially with grip strength-left, and in multivariate multiple regression analysis, the most predictive variable was grip strength-left for trunk extensors and lateral endurance. Since 94.7% of FM patients have the dominant side on the right, the non-dominant grip strength of the patients showed the strongest correlation. The non-dominant side is weaker than the dominant side. Therefore, the non-dominant side may have used more core strength instead of its own extremity strength in its functions. Grip strength is often assessed because it not only reflects the condition of the hand but also gives insights into the overall strength of the upper limb muscles. Grip strength is essential for holding various hand-held objects. In the present study, the effect of the core on grip (especially the non-dominant side) in FM was observed.
Reduction in muscle strength is an important factor in chronic pain and muscle fatigue in FM patients [36]. Compared to healthy controls, a decrease in muscle strength was observed in the lower and upper extremities in FM patients [37]. Mannerkorpi et al. [38] reported that one out of every 3 women with FM experienced problems in simple daily activities due to upper extremity strength insufficiency. This decrease in strength of the extremities may be due to the decrease in endurance of the core region. Ng et al. [39] stated that the highest activity in the core extensor endurance test was in the multifidus muscle. The transversus abdominis, external oblique, and internal oblique muscles are activated in the core lateral muscle endurance test [40]. The results of the present study can be taken as a reference in determining which muscles are more specifically related to core extensor and lateral muscle endurance in FM patients, for whom there is very little information about specific muscle effects.
Widespread muscle tenderness and pain are seen in FM patients. Evaluation of tender points is a method frequently used in the evaluation of physical findings of FM [41]. Pain and pressure pain sensitivity were found to be associated with physical functions in individuals with FM [42]. Pain negatively affects physical functions in daily life, and this effect on physical functions causes a decrease in muscle strength [43]. The decrease in the strength and endurance of the core muscles leads to physiological stress on the passive structures of the spine. This may reduce functional performance by causing pain in the body [44]. In the present study, core muscle endurance was found to be associated with pain and the pressure pain threshold in women with FM. Borghuis et al. reported that the trunk muscles are activated early and synergistic muscles are activated late, which can cause dysfunction and pain [45]. But why did women with FM who had low core flexor and lateral (especially right) muscle endurance feel pain more intensely and have lower pressure pain thresholds? This situation needs to be clarified in future studies. The mechanism underlying the effect of the decrease in core lateral muscle endurance on the increase in the number of painful areas and the decrease in the pressure pain threshold should be investigated in more detail.
The ultimate aim of the studies is to find variables that healthcare professionals can use to identify factors that are at high risk of causing greater problems for individuals in the future (e.g., during physical examinations) [46]. For this reason, we think that the present study is important in terms of the information it provides to experts about which muscle group can cause which problems in individuals with FM.
The strength of the present study is that it is the first study to examine the relationship between core stabilization and functional status of the extremities and pain in individuals with FM. The information obtained can be helpful in determining the exercises to focus on in treatment.
Study limitations
There were some limitations in the present study. It is very difficult to generalize with weak to moderate correlation findings. For this reason, clearer findings might have been obtained if there had been a healthy control group. The lack of psychological factors (depression, anxiety, etc.) is another limitation. Moreover, if the endurance of the diaphragm (superior) and pelvic floor and hip girdle (inferior) as well as the anterior, lateral and posterior muscles forming the core region had been evaluated, clearer results concerning the functional impact might have been obtained.
In future studies, we suggest conducting a detailed examination of FM symptoms that may affect the core muscle endurance compared to healthy controls. In addition, examining the effects of endurance exercises for the core extensor muscle group on lower and upper extremity functionality, core lateral muscle endurance exercises on upper extremity functionality, and core flexor and lateral muscle endurance on the number of painful areas and pressure pain threshold could provide important information for physiotherapists working in this field.
Conclusions
In the present study, core muscle endurance is associated with upper and lower extremity functional level, aerobic capacity, and pain parameters in women with FM. While lower extremity functionality was related especially to core extensor muscles, both core extensor and core lateral muscle endurance levels were found to be related to upper extremity functionality (especially the left side). In addition, women with FM who had less core flexor and lateral (especially right) muscle endurance felt pain more intensely and had lower pressure pain thresholds.